About this course:
The learning activity aims to increase knowledge of registered nurses (RN) and licensed practical nurses (LPNs) regarding arthritic disease with a focus on osteoarthritis (OA), rheumatoid arthritis (RA), psoriatic arthritis, axial spondyloarthritis, gout, and juvenile idiopathic arthritis (JIA).
Course preview
Arthritis
After completing this activity, learners will be prepared to:
differentiate among the types of arthritis by clinical presentation and treatment
distinguish the role of pathophysiology in the development of symptoms in patients experiencing arthritis, including OA, RA, psoriatic arthritis, axial spondyloarthritis, gout, and juvenile arthritis
compare and contrast risk factors for the development of each of the described forms of arthritis
identify findings of diagnostic procedures used for arthritis that indicate specific arthritic disorders
plan patient education for various forms of arthritis
interpret current research trends in arthritis that are expected to impact the future incidence, severity, and treatment of arthritis
Background
Arthritis is a leading cause of disability in the United States. Currently, nearly 54 million adults in the United States are affected by arthritis in their joints and organs. Arthritis affects one in every five adults, and this number is projected to grow. There are several arthritis-related conditions, as arthritis simply means inflammation of the joint. Common conditions are OA, RA, psoriatic arthritis, axial spondyloarthritis, gout, and juvenile arthritis (Centers for Disease Control and Prevention [CDC], 2024a; National Institute of Arthritis and Musculoskeletal and Skin Diseases [NIAMS], 2022). The most common type of arthritis is OA (CDC, n.d.).
Anatomy and Physiology
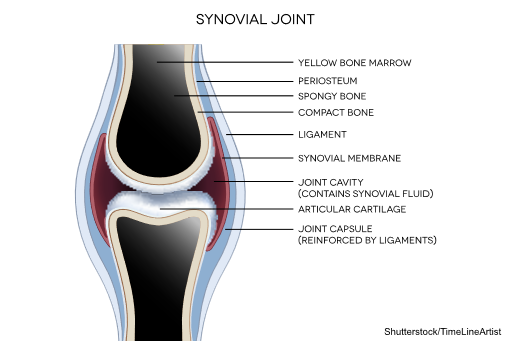
The human body contains bones, cartilage, and joints to facilitate movement. Joints that do not move are called synarthrosis; those with limited movements, such as the symphysis joint, are referred to as amphiarthrosis. Diarthrosis joints move freely and may be categorized as ball-and-socket, pivot, hinge, saddle, plane, or condyloid joints (refer to Figure 1). These are synovial joints and contain articular cartilage on the surface of the bones (refer to Figure 2). Articular cartilage contains connective tissue with an extracellular matrix comprised of water, proteoglycans, ground substance, and collagen. Amino acids and disaccharides are found in the proteoglycans, allowing for elasticity, stiffness, and movement. The joint capsule is a fibrous connective tissue that covers and stabilizes the joint. The synovial membrane surrounds the joint capsule and is responsible for secreting synovial fluid, which serves as a buffer in preventing friction or rubbing of the bones, protecting them during movement. Synovial fluid is also housed in bursae, allowing the tendons to move freely. Synovial fluid and articular cartilage collaborate in reducing friction in the joint throughout mobility. Inflammation or wearing down of any part of the joint can contribute to the discomfort associated with arthritis (Scanlon & Sanders, 2019).
Figure 1
Types of joints
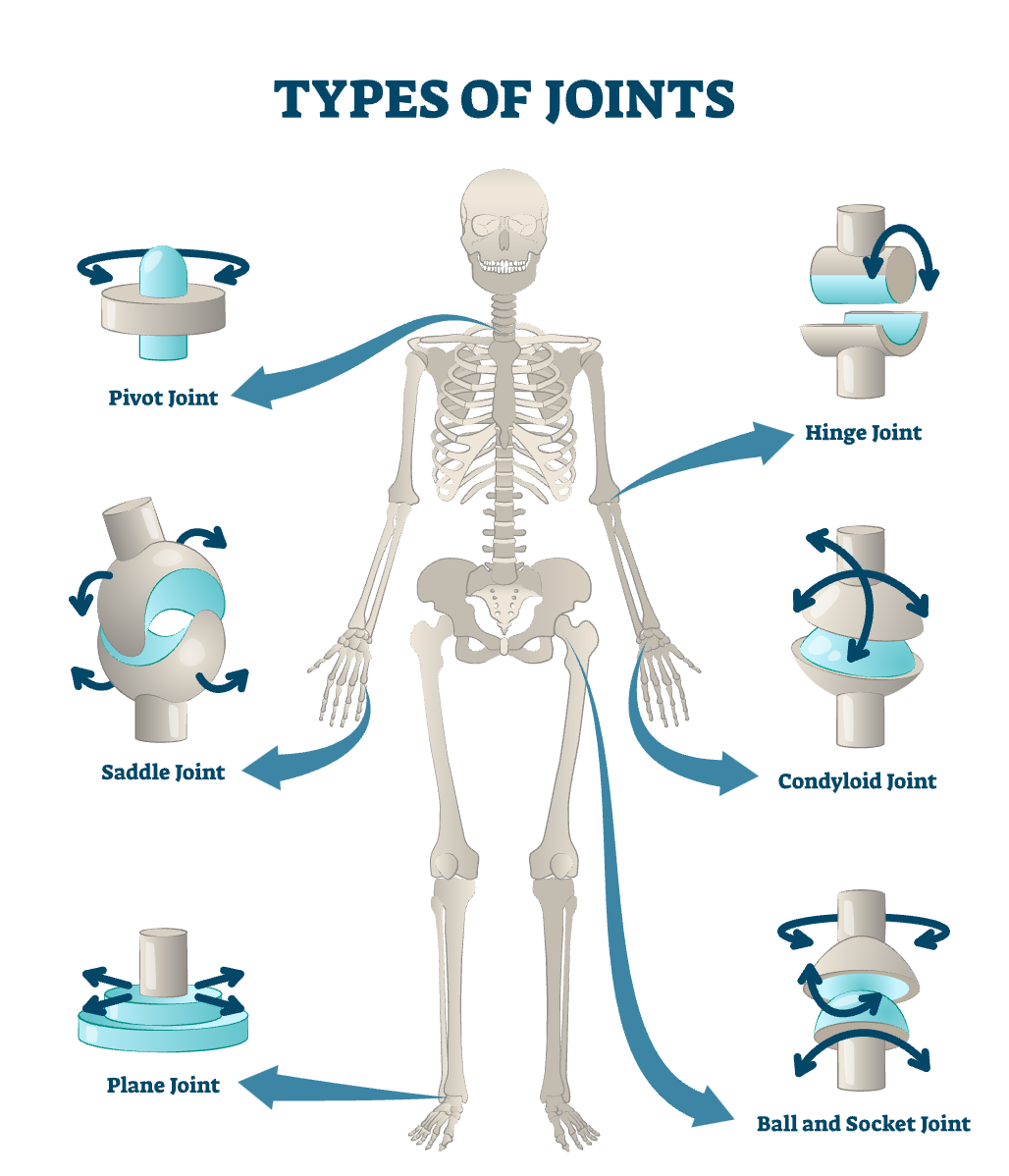
Figure 2
Close-up of synovial joint
Osteoarthritis
OA alters the entire joint due to biologic, chemical, and viscoelastic changes in the tendons and ligaments. The changes occur gradually as the articular cartilage ages. As the articular cartilage is worn down, the cushioning is decreased, and the protection of the joint is lost. Once this occurs, or if the articular cartilage is damaged, osteophytes form, causing pain and reduced range of motion (ROM). Osteophytes are also known as bone spurs. In addition, the joint’s surface becomes rough, causing the patient stiffness and instability with movement. When the damage begins, the cartilage will have more water and proteoglycans, weakening the collagen. Cytokines are released, causing further joint damage. The disease may be primary or idiopathic, with no precipitating illness related to the OA, or secondary due to previous joint injury, overuse, or inflammation. OA may be further complicated by the development of Bouchard’s nodes (refer to Figure 3) and the overproduction of synovial fluid, exacerbating pain and restricting movement. As this occurs, the patient may use their affected digit or extremity less, causing atrophy in the neighboring muscles and further weakness. Ligaments may become edematous and fibrotic, which continues to potentiate the pain and limit movement. The large and weight-bearing joints are most affected: knees, hips, hands, and spine (Loeser, 2023; Rogers, 2023; Scanlon & Sanders, 2019).
Risk Factors/Protective Features
OA is ubiquitous; currently, approximately 80% of individuals in the United States over the age of 65 have radiographic signs of OA. This condition has resulted in moderate to severe disability in 34 million individuals (Rogers, 2023). Risk factors for OA include older age, elevated body mass index (BMI), joint injury, genetics, and anatomic joint factors, such as the shape of the hip joint (Loeser, 2023). While structural changes may occur prior to 50 years of age, most...
...purchase below to continue the course
Signs and Symptoms
OA worsens over time. As the disease progresses, patients commonly experience pain, decreased ROM, tenderness to touch, and swelling. Although patients may report decreased pain while at rest, they may also experience joint pain at night and morning stiffness. The pain is typically described as aching and being difficult to localize. In addition, patients may experience crepitus and grinding in the affected joints due to the breakdown of cartilage. As the condition progresses, signs and symptoms have a greater impact on an individual’s quality of life, causing severe restrictions, joint deformity, muscle weakness, and instability of the joint. Because of this, individuals with OA have more comorbidities associated with a sedentary lifestyle (Rogers, 2023).
Diagnosis
Diagnosing OA requires a comprehensive history and physical exam. The patient will typically present with pain and stiffness at the site. The health care provider may identify alterations in the joints’ mobility, strength, and size on examination. The diagnoses can be made without laboratory or radiographic images in individuals with classic findings who are in an at-risk category (Doherty & Abhishek, 2024).
Other manifestations that can lead to diagnostic certainty include progressive onset, absent constitutive symptoms, and intermittent pain with variable intensity. If morning stiffness lasts more than 30 minutes, the individual should undergo further evaluation for the possibility of RA. Expected findings of OA on physical exam include swelling, deformity, muscle atrophy, joint line tenderness, crepitus, limited ROM, muscle weakness, and absence of warmth. While routine imaging is not necessary, it is helpful in diagnostic uncertainty and ruling out other conditions. Radiographs are used most often and may show evidence of OA, which includes joint-space narrowing, subchondral sclerosis or cysts, bone end deformity, or visible osteophytes (Doherty & Abhishek, 2024).
Figure 3
Heberden’s and Bouchard’s nodes

Treatment/Management
Nonpharmacologic
Caring for patients with OA requires a holistic approach. Patients may benefit from exercise programs to alleviate pain, improve functioning, and prevent further disability related to their OA. Exercise and muscle-strengthening activities are helpful to patients with OA. Patients may utilize assistive devices, such as a cane or walker, to help with mobility. If weight-bearing joints, such as the knees, are impacted, individuals with an elevated BMI may benefit from participating in a weight loss program (Deveza, 2024; Kolasinski et al., 2020; Rogers, 2023). Weight loss and exercise have been shown to be two of the most vital nonpharmacologic therapies to treat OA of the knee. Nutritional recommendations may include oily fish twice a week, vitamin D from safe sun exposure, dietary sources, or supplementation, increased long-chain n-3 fatty acid intake, and increased vitamin K. If nonpharmacologic measures coupled with medications do not help the patient, surgical joint replacement may be recommended (Rogers, 2023).
Pharmacologic
Medication management for OA focuses primarily on pain management and reducing inflammation. These medications should be used as needed, since none of the therapies are disease-modifying. In individuals with one or a few symptomatic joints, topical nonsteroidal nonsteroidal anti-inflammatory drugs (NSAIDs), such as diclofenac (Voltaren), have similar efficacy and a better safety profile than oral NSAIDs. Oral NSAIDs are recommended in individuals without an adequate response to topical NSAIDs, those with multiple joints involved, or those with OA of the hip (Arcangelo et al., 2022; Deveza, 2024). Examples of NSAIDs used for OA include ibuprofen (Advil, Motrin), naproxen (Aleve), celecoxib (Celebrex), and acetylsalicylic acid (ASA; Bayer Aspirin). NSAIDs work by inhibiting cyclooxygenase, thus preventing prostaglandin activity. Adverse effects include tinnitus, nausea, gastrointestinal (GI) bleeding, dyspepsia, occult bleeding, constipation, and abdominal bloating. (Arcangelo et al., 2022).
If NSAIDs are ineffective in reducing pain, patients may be given an intraarticular (IA) corticosteroid injection if they have one or two joints significantly affected by OA. Corticosteroids decrease inflammation, but they are not recommended routinely due to potential effects on the cartilage and short duration of relief. These injections are typically effective for weeks to months (Deveza & Bennell, 2025).
Duloxetine (Cymbalta) can also be used in patients with OA, either as monotherapy or in combination with NSAIDs. Duloxetine (Cymbalta) is a serotonin and norepinephrine reuptake inhibitor that reduces pain transmission in the central nervous system. While originally developed for the treatment of depression, it is approved by the US Food and Drug Administration to treat chronic musculoskeletal pain. Adverse reactions include fatigue, dizziness, nausea, somnolence, constipation, and dry mouth (Arcangelo et al., 2022; Deveza & Bennell, 2025).
Tramadol (Ultram) or other opioid medications can be used when NSAIDs are contraindicated, other treatment modalities have failed, or the patient is not a surgical candidate. Opioids are used as a last resort due to the risk of dependency and abuse and are not intended for chronic pain management. Adverse effects include dizziness, headaches, drowsiness, confusion, hypertension, peripheral edema, flushing, dry mouth, visual disturbances, nasal congestion, constipation, nausea, vomiting, dyspepsia, urinary frequency, urinary retention, hyperglycemia, and pruritus (Arcangelo et al., 2022).
Acetaminophen (paracetamol) is often not effective for monotherapy to treat OA, although it may be used for short-term, episodic use (Kolasinski et al., 2020).
Rheumatoid Arthritis
Pathophysiology
RA is a systemic, chronic, autoimmune disorder that prompts the immune system to react by causing inflammation in the synovial membrane; in turn, patients will feel joint stiffness and pain. The immune system targets the synovial membrane as it would an invader. This causes the activation of T cells, the release of cytokines (including tumor necrosis factor [TNF] and interleukin-1), and the formation of antibodies. Genetically, individuals at greater risk of developing RA will express the human leukocyte antigen (HLA)-DRB1 gene, which can impact the immune response related to synovial inflammation. RA causes loss of the synovial fluid and calcification of the joint; over time, this causes a decrease in the ROM. RA also has systemic effects; it can damage the heart and vasculature, increasing the risk for myocardial infarction and stroke (Rogers, 2023).
Locally, the autoimmune response includes the activation of neutrophils, macrophages, and lymphocytes. The neutrophils and macrophages release lysosomal enzymes, which destroy the joint cartilage. The inflammation continues cyclically, eventually impacting the synovial cells and subsynovial tissues, causing hyperplasia and vasodilation. Vasodilation contributes to the redness and warmth and promotes increased capillary permeability, causing edema. New vasculature is created, and inflammation worsens by developing a pannus, which is synovial tissue proliferation. This destroys cartilage and bone, contributing to the decreased ROM and joint instability. Although patients may experience periods of exacerbation and remission, RA is a progressive and irreversible condition (Firestein & Guma, 2023; Rogers, 2023).
Risk Factors/Protective Features
Currently, RA affects about 1% of the population (Firestein & Guma, 2023). Genetics related to joint inflammation and overactivation of the immune system are correlated with a diagnosis of RA. Other risk factors include the environment and cigarette smoking. Adults in their sixth and seventh decades are at the greatest risk for developing RA; individuals assigned female at birth have a greater lifetime risk of developing RA than individuals assigned male at birth (Rogers, 2023). Lifestyle factors, in addition to cigarette smoking, such as elevated BMI, poor diet, and physical inactivity, can increase an individual’s risk of developing RA. Other environmental causative factors include exposure to viruses and bacteria in the gut, occupational exposure to inhalants, and pollution. Because of the debility that RA causes individuals, significant research has been focused on disease prevention, which includes preventive immunomodulating therapies and modifiable risk factors for individuals at high risk for RA (England & Mikuls, 2024).
Signs and Symptoms
While OA may have unilateral joint involvement, individuals with RA characteristically have bilateral joint involvement and disability. Most causes have an insidious onset, while a smaller percentage, around 15%, may present with an acute onset (Rogers, 2023). Systemic signs and symptoms such as fever, weakness, fatigue, weight loss, and generalized aches and stiffness are typically the first presentation, followed by more local signs and symptoms such as joint tenderness, pain, and stiffness (CDC, 2024b; Rogers, 2023). Joint stiffness in the morning, commonly caused by synovitis, may last 30 minutes to several hours. The most common sites of RA include the wrists, metacarpophalangeal joints, and proximal interphalangeal joints. RA affects these smaller joints initially, followed by larger joints as the condition progresses (Rogers, 2023). The hands may become deformed, and patients may exhibit swan-neck deformities and ulnar deviation due to edema, joint destruction, or subluxation (refer to Figure 4; England, 2025; Rogers, 2023). In addition, patients may experience Boutonniere deformities, which present with hyperextension of the distal interphalangeal joints and flexion of the proximal interphalangeal joints. Over time, with long-standing RA, the cervical spine may become impacted, causing neck discomfort, occipital headaches, and muscle weakness in the upper arms (England, 2025).
Figure 4
Swan-neck deformity

RA has systemic involvement; thus, systemic signs and symptoms are likely present. Patients may experience fatigue, anorexia, weight loss, general aching, and stiffness (Rogers, 2023). RA has been noted to affect the heart, lungs, and eyes. Patients may report a low-grade fever, dry mouth, gum inflammation, shortness of breath, dry eyes, and photosensitivity. The heart and blood vessels may be inflamed, and serum laboratory testing may indicate anemia. The patient may have rheumatoid nodules, which are small lumps surrounding small blood vessels located on or near bony prominences (England, 2025; Rogers, 2023).
Diagnosis
A diagnosis of RA is confirmed using a physical assessment, serum laboratory tests, and imaging (CDC, 2024b). A history and physical evaluation should be performed to assess for pain, disability, joint tenderness, edema, and temperature changes. The joint may have a spongy-like feel due to inflammation and synovial thickening (Rogers, 2023). The serum laboratory tests will include the erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), rheumatoid factor (RF), and anticitrullinated peptide antibodies (ACPA; Baker, 2024; Rogers, 2023). However, RF is not diagnostic, as only 45% to 75% of individuals with the condition may have a positive RF (Rogers, 2023). An elevated ESR and CRP indicate the presence of inflammation. If the laboratory findings demonstrate a high RF, the patient is likely experiencing systemic effects of RA (Baker, 2024).
Radiographs are recommended for all patients with suspected RA. Radiographs may be normal in the early stages of RA, and changes on radiographs are not required for diagnosis. Other imaging tests include ultrasound and magnetic resonance imaging (MRI), which may be more sensitive at detecting bony erosion, a later manifestation of RA. Imaging tests are utilized to assess progression and the effectiveness of RA treatment. Synovial fluid may be examined for markers of inflammation (Baker, 2024).
Treatment/Management
Nonpharmacologic
The goal of treatment for individuals with RA is the prevention of injury to the joint and controlling synovitis. This is achieved through early diagnosis, specialist care, early disease-modifying antirheumatic drug (DMARD) initiation, and anti-inflammatory medications. Individuals with RA should be educated on the benefits of rest, physical exercise, occupational therapy (OT), psychosocial interventions, and proper body mechanics. Patients should also be encouraged to participate in smoking cessation and maintain a healthy weight (CDC, 2024c; Moreland & Cannella, 2024). Surgery may be an option for individuals with severe disease that includes intractable pain, disability due to destruction of the joint, and impending tendon rupture (Moreland & Cannella, 2024).
Pharmacologic
RA treatment aims to enhance the patient’s mobility by decreasing inflammation and slowing the progression of disability. Early medication initiation is desired due to the potential responsiveness of T cell–dependent pathways when combating inflammation (Moreland & Cannella, 2024). Individuals may achieve remission with medication management, and remission without this is rare. Subsequently, achieving remission does not preclude the patient from ongoing erosive damage caused by RA (England, 2025). Drug classes may include synthetic and biologic DMARDs, NSAIDs, and corticosteroids. DMARDs suppress the immune system by combating proinflammatory mediators such as TNF, B-cells, T cells, and IL-1 (Table 1). NSAIDs, such as meloxicam (Vivlodex) and naproxen (Naprosyn), and corticosteroids are given to decrease inflammation and pain; however, these medications do not slow the progression of RA (Arcangelo et al., 2022).
Table 1
Disease-Modifying Antirheumatic Drugs
Conventional synthetic DMARDs | |
Methotrexate (Trexall) = first-line treatment and most commonly prescribed |
|
Hydroxychloroquine (Plaquenil) |
|
Sulfasalazine (Azulfidine) |
|
Leflunomide (Arava) |
|
Targeted synthetic DMARDs | |
Tofacitinib (Xelijanz) |
|
Biologic DMARDs | |
TNF Inhibitors: Interfere with TNF to prevent the release of chemical and immunologic factors that damage joints in RA (and other inflammatory disorders). The medications are each a unique monoclonal antibody that binds to TNF. | |
Etanercept (Enbrel) |
|
Adalimumab (Humira) |
|
Golimumab (Simponi) |
|
Infliximab (Remicade) |
|
Certolizumab pegol (Cimzia) |
|
Non-TNF inhibitor biologics | |
Rituximab (Rituxan) |
|
Abatacept (Orencia) |
|
Tocilizumab (Actemra) |
|
(Arcangelo et al., 2022; Cohen & Mikuls, 2024)
Psoriatic Arthritis
Pathophysiology
Psoriatic arthritis is a chronic disease in which the immune system attacks the integumentary system (including skin and nails), joints, axial skeleton, and cardiovascular system (Stober, 2021). This is thought to be caused by both adaptive and innate immune responses. Abnormalities of T cells, monocytes, neutrophils, synovial fibroblasts, IL-23/IL-17 and TNF pathways, synovial fluid cytokines, and synovial tissue cytokines are all part of the pathogenesis of psoriatic arthritis. T cells are present in the skin and joints of individuals with psoriatic arthritis. However, it is unknown if these activated T cells are from inflammation or the cause of the arthritis (Gladman & Ritchlin, 2024b). Enthesitis, inflammation where the ligaments, tendons, and joint capsules attach to the bone, also plays a key part in psoriatic arthritis. Osteoblasts, osteocytes, and osteoclasts also orchestrate abnormal remodeling of cartilage and bone. The resulting damage contributes to pain, joint destruction, and erosions (Gladman & Ritchlin, 2024b; Stober, 2021).
Risk Factors/Protective Features
The incidence of psoriatic arthritis per year is approximately 6 per 100,000 individuals, affecting both sexes equally (Gladman & Ritchlin, 2024a). Individuals with a genetic predisposition to psoriatic arthritis are at a particularly heightened risk when experiencing significant stress (Stober, 2021). Environmental factors, such as bacterial infections, viral infections, and trauma, have all been associated with the development of psoriasis and psoriatic arthritis. Additionally, up to 30% of patients with psoriasis will develop psoriatic arthritis (Gladman & Ritchlin, 2024b). Most patients with both psoriatic arthritis and psoriasis will first develop skin symptoms. Some will present with skin and arthritis symptoms simultaneously, and about 10%–15% will present with arthritis first (Singh et al., 2019). Clinical manifestations of psoriasis that are associated with an increased risk of psoriatic arthritis are nail dystrophy, scalp lesions, and gluteal/perianal lesions (Gladman & Ritchlin, 2024a).
Signs and Symptoms
The areas that individuals with psoriatic arthritis are most likely to experience signs and symptoms of are the peripheral joints, skin and nails, axial skeleton, entheses, and dactylitis. Enthesis is where the joint capsules, ligaments, and tendons attach to bone, and dactylitis is the swelling of a whole digit. The majority of individuals have clinical manifestations in more than one of these domains, and around a third have clinical manifestations involving at least three domains. Individuals with psoriatic arthritis are likely to experience systemic inflammation, such as fatigue, which is reported in approximately 22% of individuals. Polyarthritis is more common than oligoarthritis, although patients with psoriatic arthritis may present with several different clinical patterns such as distal arthritis, asymmetric oligoarthritis, and arthritis mutilans. While not the most common patterns, distal arthritis and arthritis mutilans are more specific to psoriatic arthritis. Distal arthritis is distal interphalangeal joint involvement, and arthritis mutilans is destructive and deforming arthritis. Nail lesions are more common in patients with psoriatic arthritis and psoriasis (up to 90%), compared to patients with only psoriasis. These changes include pits, onycholysis, splinter hemorrhages, and hyperkeratosis (Gladman & Ritchlin, 2024a).
Diagnosis
Psoriatic arthritis is diagnosed based on the patient’s physical assessment, serum laboratory findings, and imaging results. Laboratory findings are not specific, and there are none that differentiate this type of arthritis from other forms or other autoimmune conditions.. Radiograph typically has distinct findings that are not characteristic of other inflammatory arthritis, such as simultaneous erosive changes with new bone formation. The diagnosis should be at the top of the list of differentials in a patient who presents with a history of psoriasis and inflammatory arthritis (Gladman & Ritchlin, 2024a).
Treatment/Management
Nonpharmacologic
The goal of treating psoriatic arthritis is to decrease pain and inflammation and protect the skin and joints. Early diagnosis and intervention with therapy are keys to improving long-term outcomes. Treatment is guided by the domains affected, such as peripheral joints, skin and nails, axial skeleton, entheses, and dactylitis. Patients may experience relief from discomfort by participating in physical therapy (PT), OT, increasing physical activity, weight loss, massage therapy, and smoking cessation. Low-impact exercises, such as swimming, are preferred. Individuals may also try alternative therapies such as acupuncture. Of these recommendations, smoking cessation has the highest level of evidence for recommendation (Singh et al., 2019). Weight loss may specifically aid in an increase in pharmacologic response (Gladman & Orbai, 2025; Singh et al., 2019).
Pharmacologic
For patients with psoriatic arthritis who are treatment-naïve, a TNF inhibitor, which is a biologic DMARD, is recommended first line. Oral small molecule medications (nonbiologic DMARDs), such as methotrexate (Trexail), sulfasalazine (Azulfidine), cyclosporine (Neoral), leflunomide (Arava), and apremilast (Otezia), may be used in patients without severe disease or severe psoriasis and those who prefer oral medication (Singh et al., 2019).
Axial Spondyloarthritis
Pathophysiology
Axial spondyloarthritis is an inflammatory disease in the axial skeleton that causes extensive pain and disability (Ritchlin & Adamopoulos, 2021). The condition comprises two subsets: ankylosing spondylitis (AS) and nonradiographic axial spondyloarthritis (nr-axSpA). AS does not have a clear pathogenesis; however, the presence of mononuclear cells points to immune system dysfunction. The inflammation of the spine, including associated pain, contributes to sacroiliitis (inflammation of the sacroiliac joint), an axial spondyloarthritis symptom. Typically, one or both sacroiliac joints are inflamed and painful. The specific location of the pain is at the entheses, where the ligaments and tendons attach to the bone. Events contributing to the pathogenesis of AS involve interactions between genetics, immune responses, the bowel, peripheral entheses and joints, and the axial skeleton and its entheses (Ermann, 2024).
Risk Factors/Protective Features
Currently, 1.5 million Americans have axial spondyloarthritis. Patients tend to be younger, with an average onset of disease at 28. AS is more common among individuals assigned male at birth, while nr-axSpA is equally prevalent in both sexes (Deodhar, 2020). HLA-B27 is a significant genetic precursor to axial spondyloarthritis. Most patients with axial spondyloarthritis carry the HLA-B27 gene. Common coexisting conditions include other systemic inflammatory diseases such as psoriasis, IBD (Crohn’s disease and ulcerative colitis), enthesitis (inflammation of the entheses), and uveitis. These conditions are often described as extramusculoskeletal manifestations of axial spondyloarthritis instead of comorbidities (van Tubergen, 2024).
Signs and Symptoms
The hallmark patient presentation with axial spondyloarthritis consists of back pain and stiffness for over 3 months (Deodhar, 2020). The back pain tends to occur in the sacroiliac joints, peripheral joints, entheses, and digits. Symptom onset is typically before 40 years of age. Pain characteristically has an insidious onset, improves with exercise, does not improve with rest, and worsens at night, with improvements upon awakening. Some patients experience peripheral spondyloarthritis (pain, edema, and stiffness in the extremities). Excessive lumbar lordosis (sway-back), and thoracic kyphosis may be present, particularly as the disease worsens. If the kyphosis is severe, the patient may experience heightened pain levels and difficulty balancing, contributing to an increased risk of cervical fracture. Patients may also experience fatigue, which can be as debilitating as the pain, as well as poor sleep due to pain (van Tubergen, 2024).
Diagnosis
Diagnosing axial spondyloarthritis is based on criteria established by the Assessment of Spondyloarthritis International Society. The criteria are multifaceted and include physical assessment findings, patient history, genetic testing, serum, and radiologic findings. The patient must experience back pain for over 3 months, be less than 45 years old, and have the presence of HLA-B27 and sacroiliitis. In addition, they may have another form of arthritis, IBD, psoriasis, uveitis, enthesitis, dactylitis, respond to NSAIDs treatment, a family history, and an elevated CRP or ESR (Deodhar, 2020). Sacroiliitis may be present on MRI or radiograph. Radiologic findings may include joint-space narrowing, sclerosis, and erosive changes (van Tubergen, 2024).
Treatment/Management
Nonpharmacologic
Patients should be encouraged to participate in fitness programs focusing on back exercises. Patients may benefit from OT and/or PT. Exercise has been shown to improve quality of life, and a lifetime exercise program is recommended. Patient education regarding exercise and posture-training programs, smoking cessation, psychosocial support, and depression screening are additional nonpharmacologic recommendations. When lifestyle changes and medication do not provide relief, patients may rarely require surgical intervention, such as total hip replacement, cervical fusion, or corrective wedge osteotomy (van Tubergen, 2025).
Pharmacologic
The initial medication therapy recommended for individuals with axial spondyloarthritis is NSAIDs. No specific NSAID has shown increased efficacy in the condition over others, but individuals should be tried on one for at least two to four weeks prior to assessing efficacy and switching to an alternative. Maximum dosage of the selected NSAID is often needed for management, which requires close monitoring of NSAID adverse effects, such as gastrointestinal, cardiovascular, and kidney concerns. A majority of individuals report significant relief from NSAIDs, and these are recommended to be used on demand for symptoms, which means taking them daily for many individuals (van Tubergen, 2025). If NSAIDs are ineffective, patients may be prescribed biologics, such as TNF inhibitors and interleukin (IL)-17 inhibitors (van Tubergen, 2025).
Gout
Pathophysiology
Patients with gout have high levels of uric acid and urate crystal deposits in the bones, joints, and soft tissues (Merriman, 2024; Rogers, 2023). These high levels of serum urate are characteristic of the development of this condition. Hyperuricemia is defined as greater than 7 mg/dL in individuals assigned male at birth and 6 mg/dL in individuals assigned female at birth (Rogers, 2023). This may be caused by overproduction or impaired excretion by the kidneys or gut. While individuals must have hyperuricemia to develop gout, most individuals with hyperuricemia do not develop gout. Inflammatory responses and the formation of monosodium urate crystals likely play a role in the difference between individuals who do and do not develop this condition (Merriman, 2024). Gout occurs in stages as the disease progresses, consisting of asymptomatic disease, symptomatic disease, and symptomatic disease with complications (Rogers, 2023).
During the asymptomatic hyperuricemia phase, the patient may have high uric acid levels; however, they may not experience gout pain. In an acute gout arthritis attack, the patient will have a single joint experiencing inflammation and pain as a flare-up. The time between gout flare-ups is known as intercritical gout; if a patient is not treated, their flare-ups are more likely to increase in frequency and severity (Gaffo, 2025). Tophaceous gout is the final phase when the uric acid crystals in the joints are large and form tophi, which can promote bone erosion and joint damage (Perez-Ruiz, 2023; Rogers, 2023). The high levels of uric acid cause monosodium crystal deposits in a joint, leading to an inflammatory response when macrophages attempt to phagocytize the monosodium crystals. The more distal the joint, the cooler the temperature; uric acid crystals are less soluble in temperatures less than 37°C. As such, inflammation in the peripheral joints is expected. Micro-tophi formation further promotes the release of leukocytes and the complement cascade. The inflammation damages the cartilage and subchondral bone, resulting in pain. As the frequency of these events increases, so does the risk for chronic arthritis and tophi. After 10 years, the patient may experience chronic tophaceous gout; during this time, the patient will have more recurrent, extensive, and painful gout attacks (Hoffman & Sullivan, 2020; Merriman, 2024; Rogers, 2023).
Risk Factors/Protective Features
Individuals assigned male at birth are more likely to experience gout than individuals assigned female at birth. Other nonmodifiable risk factors include older age, Asian American groups, and genetics. Lifestyle risk factors include elevated BMI, high purine diet, and alcohol intake. Comorbid conditions that place an individual at higher risk include hypertension, diabetes mellitus, and chronic kidney disease. Medications may also increase risk, such as aspirin and diuretics (Gaffo, 2025; Rogers, 2023). Patients taking thiazide diuretics are at risk for gout due to urate reabsorption in the kidneys, which increases serum levels of uric acid. In addition, individuals assigned male at birth between the ages of 40 and 60 are at a greater risk of experiencing the clinical manifestations of gout. A diet high in high-fructose corn syrup is an additional risk factor. Once gout has been diagnosed, the risk factors for gout flares are similar. These include physiologic alterations such as trauma or surgery, environmental changes such as high temperatures or humidity, medication changes, alcohol intake, triggering foods, and hospitalization (Gaffo, 2025).
Signs and Symptoms
Patients may not experience any signs or symptoms during the asymptomatic hyperuricemia phase of gout. From there, pain may be experienced in the distal joints, such as the first metatarsophalangeal joint, midfoot, and knee. The distal joints of the lower extremities are more commonly affected. The pain may occur at night, following exercise, and after consuming alcohol, medications, or certain foods. The pain and inflammation coincide. The patient will likely experience erythema and edema at the gout attack site; in addition, the patient may experience tenderness on palpation and sensitivity to touch. Asymptomatic periods lasting months to years may separate gout flare-ups. As the frequency of the attacks increases, the patient will more likely progress into the third (intercritical gout) and fourth phases (chronic tophaceous gout). Even in intercritical gout (the time between flare-ups), crystals can continue to deposit and cause bony erosions that progress into chronic gout. Although gout signs and symptoms typically affect the distal joints, the disease has a systemic impact. It correlates with elevated BMI, metabolic syndrome, hyperlipidemia, alcohol use disorder, and renal insufficiency. Any workup for gout should consider these associated or comorbid conditions (Gaffo, 2025).
Diagnosis
Gout should be suspected when serum uric acid levels rise above 6.8 mg/dL; however, uric acid levels may normalize during a gout flare. Aspiration of synovial fluid via arthrocentesis to assess for tophaceous deposits may provide a more definitive diagnosis for gout, although this is not required for diagnosis, which can be made clinically. This would be more beneficial when a diagnosis remains uncertain. Imaging tests may further assess the impact on the joint(s). Early imaging tests may not demonstrate any changes to the joint; however, erosions and nodules become visible in time (Gaffo, 2025).
Treatment/Management
Nonpharmacologic
Lifestyle changes can enhance the management of gout. More specifically, patient education focusing on avoiding or limiting alcohol, maintaining a healthy weight, smoking cessation, and avoiding purine-rich foods will help patients with gout. Purine-rich foods include seafood, alcohol, and red meats (Clebak et al., 2020). If the joint can be temporarily placed in a splint, the patient may experience less pain (Hoffman & Sullivan, 2020).
Pharmacologic
Pharmacologic management aims to suppress pain and inflammation with a systemic anti-inflammatory agent, such as NSAIDs, glucocorticoids, colchicine (Mitigare), or interleukin 1 inhibitor. The choice of medication depends on the risk of adverse effects versus the benefits. NSAIDs, such as naproxen (Naproxen) or indomethacin (Indocin), are commonly used for flare-ups. In addition, patients may be given colchicine (Mitigare). Adverse effects include fatigue, headaches, diarrhea, nausea, and vomiting. Both systemic and IA glucocorticoids may be used for gout flares. While IA glucocorticoids may be effective, the evidence supporting their use is limited, and administration requires an experienced provider (Gaffo, 2024).
Long-term medications may be utilized if a patient experiences two or more gout attacks per year or has chronic renal disease, urolithiasis, tophi, chronic gouty arthritis, and joint damage. Allopurinol (Zyloprim) and febuxostat (Uloric) may be used for gout maintenance treatment; allopurinol (Zyloprim) is preferred as febuxostat (Uloric) has a risk of cardiovascular mortality. Adverse effects include nausea, vomiting, abdominal pain, and diarrhea. Allopurinol (Zyloprim) should be administered with food to minimize these effects. Allopurinol (Zyloprim) should not be used to treat a gout exacerbation (Arcangelo et al., 2022; Perez-Ruiz, 2025). Adverse effects include dizziness, nausea, and rash (Arcangelo et al., 2022).
Juvenile Arthritis
Pathophysiology
JIA consists of arthritis that presents prior to 16 years of age in the absence of another contributing medical condition. JIA is the most common childhood rheumatologic condition. There are several subtypes, which include systemic, oligoarticular, polyarticular-rheumatoid factor positive, polyarticular-rheumatoid factor negative, psoriatic, enthesitis-related, and undifferentiated. The cause is unknown; however, it is believed that the immune system attacks and permanently damages the joints. Specifically, TNF-alpha, IL-6, and IL-1 contribute to inflammation in the synovial membrane of the joint (American College of Rheumatology, 2025; CDC, 2024b; NIAMS, 2024).
Risk Factors/Protective Features
JIA impacts 1 in every 1,000 children (American College of Rheumatology, 2025). Although no specific risk factors have been outlined, genetics and the environment may contribute to the activation of the immune system against a child’s joints. JIA impacts children across all ethnicities and races. While most subtypes are more frequent in children assigned female at birth, enthesitis-related JIA is more frequent in children assigned male at birth, and systemic JIA is equal among sexes. The most significant risk factor is having a family member with chronic inflammatory arthritis or other autoimmune conditions (NIAMS, 2024). JIA is also more common in children with an elevated BMI, physically inactive, have second-hand smoke exposure, heart conditions, and anxiety or depression (CDC, 2024b).
Signs and Symptoms
JIA affects individuals under the age of 16. These individuals may experience periods of remission and exacerbation (i.e., flare-ups). During a flare-up, patients may experience joint pain, edema, erythema, fever, stiffness, rash, fatigue, decreased appetite, and inflammation in the eye. This may cause limping and difficulty with fine motor functions or completing activities of daily living. Patients may experience changes in their skin, such as rashes, erythematous patches, or bumps. The patient may experience changes in their growth, causing one extremity to be shorter than the other. The symptoms are correlated to the joint impacted by the inflammation and subtype. JIA should be suspected in children who have similar signs and symptoms for at least six weeks (American College of Rheumatology, 2025; CDC, 2024b; NIAMS, 2024).
Diagnosis
JIA is typically diagnosed through physical assessment, radiograph, and serum laboratory tests, most often conducted by a pediatric rheumatologist. After collecting a family and medical history, a physical assessment is performed, including an integumentary and musculoskeletal assessment, gait evaluation, ophthalmic exam (evaluating for uveitis), an abdominal assessment, and lymphatic inspection (CDC, 2024b; NIAMS, 2024).
Anticyclic citrullinated peptide (CCP) antibodies and RF may be present if a rheumatic component of the arthritis occurs, but this is rare in children with JIA. HLA-B27 may be drawn if enthesitis-related JIA is suspected. A complete blood count (CBC) may be ordered to evaluate for infection or anemia; it is not uncommon for patients with JIA to experience anemia. A metabolic panel may be ordered to assess renal and liver function (NIAMS, 2024).
Treatment/Management
Nonpharmacologic
Treating a patient with JIA requires a holistic approach. The patient may require PT and OT to promote movement, relieve pain, prevent further injuries, and strengthen muscles. The goal is to encourage patients to actively engage in their daily activities to their fullest potential. Patients may require care from a mental health practitioner to ensure that they are coping psychologically with the physical and lifestyle changes accompanying a JIA diagnosis. Patients and caregivers should be educated on the benefits of rest and exercise on psychological and physical stress and preventing future pain; swimming is recommended as an activity, as it does not stress joints. A splint may help prevent the overuse of the affected joint (NIAMS, 2024).
Patients and their caregivers should be encouraged to live life as normally as possible; they should be encouraged to participate in social activities. Summer camps and support groups for children with similar conditions can promote further coping and holistic well-being. If the patient requires accommodation for school, the health care provider may complete accommodation forms that align with Section 504 of the Rehabilitation Act. The patient and caregivers should be given information on social services to promote access to care and to acquire the necessary resources to ensure a quality of life (American College of Rheumatology, 2025; NIAMS, 2024).
Pharmacologic
Patients with JIA may experience significant symptom management from a sound medication regimen. The patient may take DMARDs, NSAIDs, and corticosteroids (NIAMS, 2024). The child and their caregivers should be educated about the potential adverse effects of these medications. Conventional synthetic DMARDs that may be given are methotrexate (Trexall) and leflunomide (Arava). Biologic agents include etanercept (Enbrel), adalimumab (Humira), abatacept (Orencia), infliximab (Remicade), rituximab (Rituxan), anakinra (Kineret), canakinumab (Ilaris), and tocilizumab (Actemra; American College of Rheumatology, 2025). Tofacitinib (Xeljanz), a Janus kinase inhibitor, is a more recent FDA-approved oral medication to treat JIA (American College of Rheumatology, 2025; UpToDate Lexidrug, n.d.).
Future Research
Genetic Therapy
Research is being conducted to examine whether molecular profiling may enhance treatment for RA. More specifically, researchers are exploring which genes contribute to resistance to RA treatment, potentially leading to more effective therapies (Queen Mary University, 2022). Investigations for the treatment of OA that focus on regeneration include stem cell therapy, platelet-rich plasma, and tissue gene therapy. The goal of these therapies is to repair the tissue and stimulate growth factors at the site. While none of these agents are recommended for treatment, future goals include treatment that targets pain, slow destruction, and regeneration (Yu, 2025). Beyond treatment, genetic profiling can potentially promote prevention, earlier diagnoses, and treatment of arthritis (Versus Arthritis, 2020).
References
American College of Rheumatology. (2025). Juvenile arthritis. https://www.rheumatology.org/I-Am-A/Patient-Caregiver/Diseases-Conditions/Juvenile-Arthritis
Arcangelo, V. P., Peterson, A. M., Wilbur, V. F., & Kang, T. M. (2022). Pharmacotherapeutics for advanced practice (5th ed.). Wolters Kluwer.
Baker, J. F. (2024). Diagnosis and differential diagnosis of rheumatoid arthritis. UpToDate. Retrieved April 29, 2025, from https://www.uptodate.com/contents/diagnosis-and-differential-diagnosis-of-rheumatoid-arthritis
Centers for Disease Control and Prevention. (n.d.). Arthritis. Retrieved May 1, 2025, from https://www.cdc.gov/arthritis
Centers for Disease Control and Prevention. (2024a). Arthritis basics. https://www.cdc.gov/arthritis/basics/index.html
Centers for Disease Control and Prevention. (2024b). Childhood arthritis. https://www.cdc.gov/arthritis/childhood-arthritis/index.html
Centers for Disease Control and Prevention. (2024c). Rheumatoid arthritis. https://www.cdc.gov/arthritis/rheumatoid-arthritis/
Clebak, K. T., Morrison, A., & Croad, J. R. (2020). Gout: Rapid evidence review. American Family Physician, 102(9), 533–538. https://www.aafp.org/pubs/afp/issues/2020/1101/p533.html
Cohen, S., & Mikuls, T. R. (2024). Initial treatment of rheumatoid arthritis in adults. UpToDate. Retrieved April 29, 2025, from https://www.uptodate.com/contents/initial-treatment-of-rheumatoid-arthritis-in-adults
Deodhar, A. A. (2020). Understanding axial spondyloarthritis: A primer for managed care. American Journal of Managed Care, 25(17). https://www.ajmc.com/view/axial-spondyloarthritis-primer-for-managed-care
Deveza, L. A. (2024). Overview of the management of osteoarthritis. UpToDate. Retrieved April 29, 2025, from https://www.uptodate.com/contents/overview-of-the-management-of-osteoarthritis
Deveza, L. A., & Bennell, K. (2025). Management of moderate to severe knee osteoarthritis. UpToDate. Retrieved April 29, 2025, from https://www.uptodate.com/contents/management-of-moderate-to-severe-knee-osteoarthritis
Doherty, M., & Abhishek, A. (2024). Clinical manifestations and diagnosis of osteoarthritis. UpToDate. Retrieved April 29, 2025, from https://www.uptodate.com/contents/clinical-manifestations-and-diagnosis-of-osteoarthritis
England, B. R. (2025). Clinical manifestations of rheumatoid arthritis. UpToDate. Retrieved April 29, 2025, from https://www.uptodate.com/contents/clinical-manifestations-of-rheumatoid-arthritis
England, B. R., & Mikuls, T. R. (2024). Epidemiology of, risk factors for, and possible causes of rheumatoid arthritis. UpToDate. Retrieved April 29, 2025, from https://www.uptodate.com/contents/epidemiology-of-risk-factors-for-and-possible-causes-of-rheumatoid-arthritis
Ermann, J. (2024). Pathogenesis of spondyloarthritis. UpToDate. Retrieved April 30, 2025, from https://www.uptodate.com/contents/pathogenesis-of-spondyloarthritis
Firestein, G. S., & Guma, M. (2023). Pathogenesis of rheumatoid arthritis. UpToDate. Retrieved April 29, 2025, from https://www.uptodate.com/contents/pathogenesis-of-rheumatoid-arthritis
Gaffo, A. L. (2024). Gout: Treatment of flares. UpToDate. Retrieved April 30, 2025, from https://www.uptodate.com/contents/gout-treatment-of-flares
Gaffo, A. L. (2025). Gout: Clinical manifestations and diagnosis. UpToDate. Retrieved April 30, 2025, from https://www.uptodate.com/contents/gout-clinical-manifestations-and-diagnosis
Gladman, D. D., & Orbai, A. (2025). Treatment of psoriatic arthritis. UpToDate. Retrieved April 30, 2025, from https://www.uptodate.com/contents/treatment-of-psoriatic-arthritis
Gladman, D. D., & Ritchlin, C. (2024a). Clinical manifestations and diagnosis of psoriatic arthritis. UpToDate. Retrieved April 30, 2025, from https://www.uptodate.com/contents/clinical-manifestations-and-diagnosis-of-psoriatic-arthritis
Gladman, D. D., & Ritchlin, C. (2024b). Pathogenesis of psoriatic arthritis. UpToDate. Retrieved April 30, 2025, from https://www.uptodate.com/contents/pathogenesis-of-psoriatic-arthritis
Hoffman, J. J., & Sullivan, N. J. (2020). Davis advantage for medical-surgical nursing: Making connections to practice (2nd ed). F. A. Davis.
Kolasinski, S. L., Neogi, T., Hochberg, M. C., Oatis, C., Guyatt, G., Block, J., Callahan, L., Copenhaver, C., Dodge, C., Felson, D., Gellar, K., Harvey, W. F., Hawker, G., Herzig, E., Kwoh, C. K., Nelson, A. E., Samuels, J., Scanzello, C., White, D., . . . Reston, J. (2020). 2019 American College of Rheumatology/Arthritis Foundation guideline for the management of osteoarthritis of the hand, hip, and knee. Arthritis & Rheumatology, 72(2), 220–233. https://doi.org/10.1002/art.41142
Loeser, R. F. (2023). Pathogenesis of osteoarthritis. UpToDate. Retrieved April 28, 2025, from https://www.uptodate.com/contents/pathogenesis-of-osteoarthritis
Merriman, T. (2024). Gout: Pathophysiology. UpToDate. Retrieved April 30, 2025, from https://www.uptodate.com/contents/gout-pathophysiology
Moreland, L. W., & Cannella, A. (2024). General principles and overview of management of rheumatoid arthritis in adults. UpToDate. Retrieved April 29, 2025, from https://www.uptodate.com/contents/general-principles-and-overview-of-management-of-rheumatoid-arthritis-in-adults
National Institute of Arthritis and Musculoskeletal and Skin Diseases. (2022). Arthritis. https://www.niams.nih.gov/health-topics/arthritis
National Institute of Arthritis and Musculoskeletal and Skin Diseases. (2024). Juvenile idiopathic arthritis. https://www.niams.nih.gov/health-topics/juvenile-arthritis
Perez-Ruiz, F. (2023). Gout. UpToDate. Retrieved April 30, 2025, from https://www.uptodate.com/contents/gout-beyond-the-basics
Perez-Ruiz, F. (2025). Gout: Pharmacologic urate-lowering therapy and treatment of tophi. UpToDate. Retrieved April 10, 2025, from https://www.uptodate.com/contents/gout-pharmacologic-urate-lowering-therapy-and-treatment-of-tophi
Queen Mary University. (2022). New study shows genes can predict response to arthritis treatment and paves the way for future drug development. ScienceDaily. https://www.sciencedaily.com/releases/2022/05/220519115305.htm
Ritchlin, C., & Adamopoulos, I. E. (2021). Axial spondyloarthritis: New advances in diagnosis and management. British Medical Journal, 372. https://pubmed.ncbi.nlm.nih.gov/33397652/
Rogers, J. L. (2023). McCance & Huether’s pathophysiology: The biologic basis for disease in adults and children (9th ed.). Elsevier.
Scanlon, V. C., & Sanders, T. (2019). Essentials of anatomy and physiology (8th ed.). F. A. Davis.
Singh, J. A., Guyatt, G., Ogdie, A., Gladman, D. D., Deal, C., Deodhar, A., Dubreuil, M., Dunham, J., Husni, M. E., Kenny, S., Kwan-Morley, J., Lin, J., Marchetta, P., Mease, P. J., Merola, J. F., Miner, J., Ritchlin, C. T., Siaton, B., Smith, B. J., . . . Reston, J. (2019). 2018 American College of Rheumatology/National Psoriasis Foundation guideline for the treatment of psoriatic arthritis. Arthritis & rheumatology, 71(1), 5–32. https://doi.org/10.1002/art.40726
Stober, C. (2021). Pathogenesis of psoriatic arthritis. Best Practice & Research Clinical Rheumatology, 35(2). https://doi.org/10.1016/j.berh.2021.101694
UpToDate Lexidurg. (n.d.). Tofacitinib: Drug information. UpToDate. Retrieved April 28, 2025, from https://www.uptodate.com/contents/tofacitinib-drug-information
van Tubergen, A. (2024). Clinical manifestations of axial spondyloarthritis (ankylosing spondylitis and nonradiographic axial spondyloarthritis) in adults. UpToDate. Retrieved April 30, 2025, from https://www.uptodate.com/contents/clinical-manifestations-of-axial-spondyloarthritis-ankylosing-spondylitis-and-nonradiographic-axial-spondyloarthritis-in-adults
van Tubergen, A. (2025). Treatment of axial spondyloarthritis (ankylosing spondylitis and nonradiographic axial spondyloarthritis) in adults. UpToDate. Retrieved April 28, 2025, from https://www.uptodate.com/contents/treatment-of-axial-spondyloarthritis-ankylosing-spondylitis-and-nonradiographic-axial-spondyloarthritis-in-adults
Versus Arthritis. (2020). Genetics and genomics help to predict and treat arthritis. https://www.versusarthritis.org/news/2020/march/genetics-and-genomics-how-research-is-helping-us-to-predict-and-treat-arthritis/
Yu, S. (2025). Investigational approaches to the management of osteoarthritis. UpToDate. Retrieved April 30, 2025, from https://www.uptodate.com/contents/investigational-approaches-to-the-management-of-osteoarthritis
Powered by Froala Editor