About this course:
This course aims to ensure that all advanced practice registered nurses (APRNs) within primary care and emergency medicine are aware of and able to implement the most up-to-date information regarding the pathophysiology, signs, symptoms, risk factors, diagnosis, and treatment of asthma in their practice.
Course preview
Asthma (for APRNs)
This course aims to ensure that all advanced practice registered nurses (APRNs) within primary care and emergency medicine are aware of and able to implement the most up-to-date information regarding the pathophysiology, signs, symptoms, risk factors, diagnosis, and treatment of asthma in their practice.
Upon completion of this module, learners should be able to:
- formulate an understanding of the epidemiology and pathophysiology of asthma and its various phenotypes
- identify the various asthma risk factors and methods for prevention
- reference the appropriate tests and evaluations used to diagnose asthma
- discuss the lifestyle changes and environmental adjustments that can be instituted to reduce the symptoms and severity of asthma
- discuss the immunotherapy options for the treatment of asthma in those with known allergies
- explore the various assessment and management guidelines available to guide practice, including the Expert Panel Report (EPR)-4 2020 updates and Global Initiative for Asthma (GINA) guidelines
- summarize nonpharmacological and pharmacological options for the management of asthma
Asthma is a chronic inflammatory airway disorder that causes the narrowing of the airways and is the most common chronic disease diagnosed in children. It is characterized by airway hyperresponsiveness and recurrent episodes of acute symptoms, such as wheezing, coughing, chest tightness, and shortness of breath (SOB), affecting approximately 262 million people and causing 455,000 annual deaths worldwide (World Health Organization [WHO], 2024). According to the Centers for Disease Control and Prevention (CDC), asthma affects approximately 25 million (7.7%) Americans. It is more prevalent in adults (8.6%) than in children (6.5%). Asthma is responsible for over 4.9 million office visits and 1.4 million emergency department (ED) visits annually. Almost 100,000 hospitalizations were attributed to asthma-related causes in 2020. Annually, asthma costs the United States over approximately $115 billion, with over 13.8 million missed school days, and almost 34% of US adults missing workdays due to asthma. Worldwide, there are an estimated 420,000 deaths annually due to asthma-related causes. In the United States in 2023, asthma-related deaths occurred in 3,264 people. Non-Hispanic Black individuals are three times more likely to die due to asthma complications than any other racial group (Allergy & Asthma Network, n.d.-b, 2025b; Asthma and Allergy Foundation [AAFA], 2025b; CDC, 2023, 2026; Czira et al., 2022; Litonjua & Weiss, 2025; Pate & Zahran, 2024).
Among patients diagnosed with asthma, 62% of adult and 50% of pediatric patients have poorly controlled symptoms. Individuals with poor control report increased disease exacerbation, more significant impact on work or school productivity, increased utilization of health care resources, and lower quality of life (QOL). Among pediatric patients, uncontrolled asthma was more prevalent in those designated as males (7.3%) compared to females (5.6%). Poor control of asthma symptoms was highest among pediatric patients aged 5–11 (46.6%), followed by those aged 0–4 (45.8%) and 12–17 (40.6%). Uncontrolled asthma is more prevalent in adult females (9.7%) than males (6.2%). Adults aged 55–64 have the highest rate of uncontrolled asthma at 65.5%, followed by those aged 35–54 at 63.4%, older than 65 at 58.4%, and those aged 18–34 at 53.3% (CDC, 2022a, 2022b; Litonjua & Weiss, 2025; Mazi et al., 2023; Pate & Zahran, 2024).
Pathophysiology
Chronic asthma symptoms are related to a combination of inflammation and airway hyperresponsiveness. Complex interactions between genetic and environmental factors influence the presence and severity of asthma. Some researchers attribute the development of asthma to a combination of atopy (a genetic tendency toward an IgE-mediated overreaction to external triggers), a familial tendency, and exposure to particular childhood upper respiratory infection(s), allergens, or triggers. The hygiene hypothesis suggests that the rise in asthma cases in the United States in recent decades is due to Western civilization being overly sanitized, reducing the number of environmental exposures and infections, changing indoor air composition, and thus altering the immune systems of children as they age (Garn et al., 2021; Rogers & Brashers, 2023).
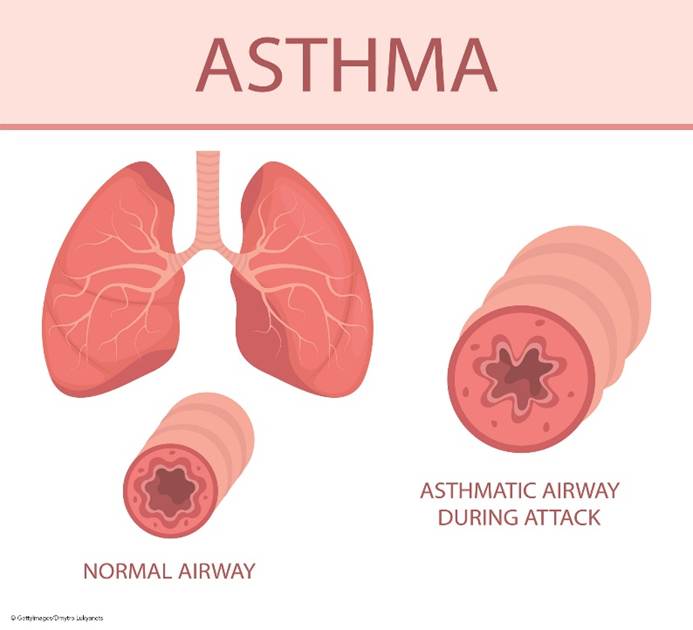
Bronchiolar inflammation and airway constriction lead to increased resistance and the hallmark symptoms of cough, wheezing, and SOB (refer to Figure 1). Inflammation may exist without obvious symptoms and can affect the trachea, bronchi, or the smaller bronchioles. The presence of inflammation is attributed to T-helper type 2 (Th2) lymphocytes, eosinophils, mast cells, and neutrophils. These cells form inflammatory infiltrates in the airway epithelium and smooth muscle, leading to remodeling, including smooth muscle hypertrophy. This hypertrophy leads to airway narrowing and increases airway reactivity to asthma triggers, such as allergens, infections, or other irritants. Airway hyperactivity is also a result of the absence of bronchoconstriction inhibitors, such as relaxing factors, prostaglandins, and endopeptidases (enzymes that metabolize bronchoconstrictors). This lack of inhibitors prolongs and intensifies the inflammatory process. In addition, the expansion of mucus-secreting glands and increased mucus-secreting cells cause increased mucus production and decreased mucus clearance, leading to mucus plugs. If left untreated, this chronic inflammation damages the respiratory tract epithelium, leading to permanent fibrosis and airway remodeling. Epithelial cells transition to mesenchymal cells, which decreases lung function and responsiveness to treatment. In addition to underlying inflammation, bronchospasms are caused by sharp contractions of the smooth muscles lining the bronchi (Allergy & Asthma Network, n.d.-b; CDC, 2024; Ortega & Chiarella, 2026a; Sinyor & Perez, 2023).
Figure 1
Airway Anatomy and Asthma Pathophysiology
Different subtypes of asthma, called phenotypes, have emerged in the last couple of decades. The most recent update of the GINA recognized these various phenotypes. However, except in patients with severe asthma, they did not feel these phenotypes correlated strongly enough with specific pathological processes or treatment responses to warrant phenotype-specific treatment algorithms (GINA, 2025b). According to GINA, some of the most common phenotype classifications include:
- allergic (eosinophilic) asthma
- nonallergic, nonatopic (neutrophilic) asthma
- cough variant and cough predominant asthma types
- adult (late) onset
- asthma with persistent airflow limitation
- asthma with obesity (GINA, 2025b)
Early-onset atopic asthma, typically diagnosed during childhood, is characterized by wheezing and associated allergies or triggers from external environmental factors, such as...
...purchase below to continue the course
About 5%-10% of all asthma patients and approximately 50%-70% of those with severe asthma fall into the eosinophilic phenotype. One subtype of eosinophilic asthma, adult late-onset, has a much later onset in the fourth or fifth decade, few to no allergies, more severe disease, and a poorer prognosis. Symptoms typically include reports of dyspnea on exertion (DOE) and chronic rhinosinusitis. Further examination and testing typically reveal fixed airflow obstruction, decreased forced vital capacity (FVC) on lung function testing (LFT), increased residual volume (“air trapping” or dynamic hyperinflation), and nasal polyposis. The definitive diagnosis for this phenotype is eosinophilia on a bronchial biopsy or an induced sputum sample. However, due to the invasiveness, cost, and difficulty in obtaining those tests, this phenotype may be estimated based on clinical presentation, LFT results, and a peripheral blood sample showing eosinophilia. Sputum analysis may benefit patients who fit the clinical picture of late-onset eosinophilic asthma. However, the difficulty and limited access to capable labs are apparent barriers to its widespread use, as only a limited number of asthma treatment centers have access to induced sputum analysis. However, GINA notes that they have been shown to reduce the risk of exacerbations in adult patients with moderate-to-severe asthma when used in conjunction with clinical management guidelines. These patients should be managed in or referred to a center experienced in this diagnostic technique. This phenotype is primarily driven by group 2 innate lymphoid cells (ILC2s), which produce IL-5 and IL-13 upon activation. Like T and B lymphocytes, ILC2s are derived from lymphoid progenitor cells but do not express antigen receptors and instead function as an essential component of the innate immune system (Allergy & Asthma Network, n.d.-a; GINA, 2025b; Heaney et al., 2021; Hussain & Liu, 2024; Porpodis et al., 2022).
Further differentiation can be made among asthma patients based on the presence or absence of eosinophilia, the age of onset (as above), the presence or absence of allergic rhinitis, the resistance to or response to certain medications (such as inhaled corticosteroids [ICS] or leukotriene receptor antagonists [LTRAs]), the presence of chronic obstructive pulmonary disease (COPD), gastroesophageal reflux disease (GERD), obesity, and vitamin D deficiency as comorbidities. These differentiations categorize endotypes, subgroups that describe the underlying pathological process, and characteristics of a particular phenotype. An increased understanding of phenotypes and underlying endotypes has impacted pharmaceutical development. As a result, new drugs are being developed that target specific molecules and disease pathways, leading to more individualized treatment, especially for those patients with severe, drug-resistant asthma (Rogers & Brashers, 2023).
Risk Factors and Prevention
Risk factors for asthma development include environmental allergens or irritants such as indoor and outdoor air pollution, dust mites, mold, chemicals, fumes, cockroach antigens, and smoke. Children with close family members diagnosed with asthma are also at an increased risk. Asthma is also more prevalent in individuals with additional allergic conditions such as eczema, food allergies, or allergic rhinitis. Individuals born prematurely or with low birth weight are also at an increased risk of developing asthma. Obese adults and children also have a higher prevalence of asthma than those with low or average body weight. It is also thought that vitamin D deficiency may play a role in the development of asthma and wheezing in children, as vitamin D suppresses Th17-mediated inflammation, IgE expression, and Th2-mediated allergic disease, and contributes to proper lung development and infection control. Statistics regarding asthma prevalence indicate that 28.2 million people in the United States are living with asthma, including 1 in 12 school-aged children. In 2023, asthma was attributed to 3,624 deaths. In children younger than 18 years of age, it is more common in males (7.0%) than in females (5.4%); in adulthood, it is more common in females (10.8%) than in males (6.5%). It is more common among non-Hispanic American Indian/Alaska Native individuals (12.5%) and non-Hispanic Black individuals (10.6%), followed by non-Hispanic White individuals (7.8%), Hispanic individuals (6.4%), and Asian individuals (4.5%). Elevated asthma rates are also related to increased poverty levels. The AAFA states that September, especially the third week, is the peak of allergy season due to the convergence of multiple triggers (e.g., ragweed, mold, back-to-school illnesses, poor indoor air quality, and extreme weather). For 2025, Detroit, Michigan; Rochester, New York; and Allentown, Pennsylvania were ranked as the worst top three cities for asthma when considering asthma-related prevalence, deaths, and ED visits (Allergy & Asthma Network, 2025b; AAFA, 2025a; CDC, 2023, 2024; Rogers & Brashers, 2023).
Asthma prevention is poorly understood; however, the GINA guidelines make the following recommendations: Children should not be exposed to tobacco smoke, including while in utero. There is conflicting data regarding the benefits of vitamin D supplementation in preventing asthma; however, when results from multiple trials are combined, there was a 25% reduction in asthma and wheezing risk in children aged 0–3, but no impact in those aged 6 or older. This benefit was observed among individuals who maintained vitamin D levels of at least 30 ng/mL throughout pregnancy to the time of delivery. One study demonstrated that high-dose fish oil supplementation during the third trimester of pregnancy decreased the prevalence of asthma and wheezing in preschool-aged children; however, the study did not define what constitutes high-dose fish oil or establish a dosing regimen. The use of acetaminophen (Tylenol) and antibiotics both during pregnancy and in children is associated with the development of asthma in children and should be avoided. Birth via vaginal delivery may also decrease the risk of asthma, as asthma rates in children born via cesarean section are higher than in those born vaginally (GINA, 2025b; Liu et al., 2022).
The adverse effects of cooking with indoor gas stoves have been studied in recent years. It is estimated that 35% of US households cook by utilizing gas appliances. Researchers analyzed 27 reports focused on the effects of gas cooking on children and found that indoor gas stoves are associated with an increased risk of childhood asthma, accounting for 12.7% of all childhood cases. This risk is comparable to that associated with secondhand tobacco smoke exposure. The risk varied with location, and researchers estimated that Illinois has the highest burden at 21.1%, followed by California at 20.1%, New York at 18.8%, and Massachusetts at 15.4% (Gruenwald et al., 2023).
Diagnosis
Diagnosing asthma can be complicated by its wide range of presentations, as discussed above. Patients may present with high levels of eosinophilic inflammation and few symptoms, severe symptoms and lower levels of eosinophilia and inflammation, or a classic presentation of eosinophilia and inflammation that correlates positively with symptom severity. The clinical signs, symptoms, and features of asthma that providers should be watchful for include a history of recurrent or chronic dry cough, wheezing, difficulty breathing, SOB, or chest tightness. Symptoms are typically worse with exertion or at night, often causing nighttime awakenings. Commonly referred to as triggers, symptoms may also increase in the context of viral upper respiratory infections (e.g., respiratory syncytial virus [RSV] or COVID-19), exposure to environmental or occupational allergens or irritants, changes in the weather (especially the presence of cold, dry air), laughing or crying spells, high-stress, exercise, and the presence of GERD. The AAFA also includes smoke and air pollution as potential triggers and lists potential allergens, including dust mites, cockroaches, mold, pet fur/dander, mice, and pollen. Additional triggers for specific patients may include medications (such as aspirin, other nonsteroidal anti-inflammatory drugs [NSAIDs], or nonselective beta-blockers), grasses, flowers, or sulfites (AAFA, 2024; National Heart, Lung, and Blood Institute [NHLBI], 2020a, 2024; Ortega & Chiarella, 2026a). Figure 2 provides more information for patients with asthma regarding possible triggers and how best to avoid them.
Figure 2
Common Asthma Triggers
(NHLBI, 2021)
The most recent GINA report states that asthma diagnosis should be based on history and symptom patterns, as well as evidence of variable expiratory airflow limitation via spirometry (FVC and forced expiratory volume [FEV1]) or peak expiratory flow (PEF or peak flow) measurements with a reversibility test. For further details regarding GINA’s diagnostic criteria, refer to Table 1 (GINA, 2025b).
Table 1
GINA Diagnostic Criteria, Age 6+
Diagnostic Feature | Criteria for Diagnosis |
History of variable respiratory symptoms | |
Wheeze, SOB, cough, and chest tightness (descriptions may vary based on age, culture, etc.) |
|
Confirmed variable expiratory airflow limitation | |
Documented excessive variability in lung function (one of the tests below) AND documented expiratory airflow limitation |
|
Positive bronchodilator reversibility test (more likely to be positive if bronchodilator is withheld before the test; short-acting beta agonist (SABA) ≥ 4 hours, twice daily long-acting beta-agonist (LABA) 24 hours, and once daily LABA 36 hours |
|
Excessive variability in twice-daily PEF over 2 weeks |
|
Significant increase in lung function after 4 weeks of inhaled corticosteroid (ICS) treatment |
|
Positive exercise challenge test |
|
Positive bronchial challenge test (usually adults only) |
|
Excessive variation in lung function between visits (less reliable; good specificity with poor sensitivity) |
|
(GINA, 2025b)
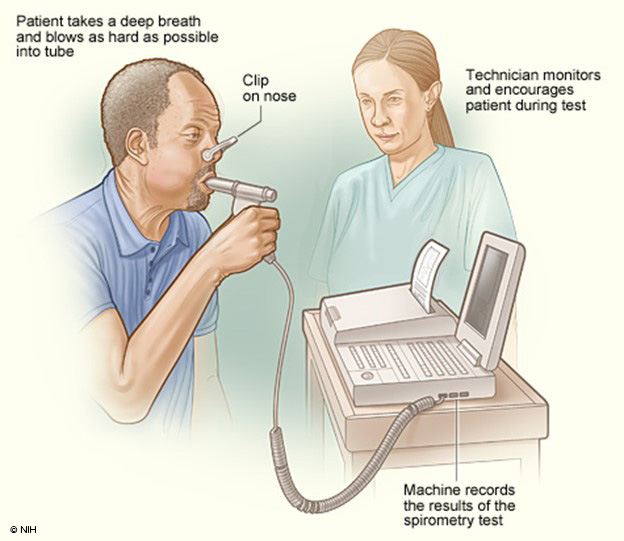
The National Asthma Education and Prevention Program (NAEPP) last published full guidelines in 2007, called the Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma (EPR-3). In 2020, the EPR-4, a focused update on six priority topics, was released. This report recommends that patients aged 5 years or older suspected of having asthma be tested with spirometry before and after a dose of SABA medication (NHLBI, 2020a). Spirometry testing (refer to Figure 3) is one of the most commonly used tests to measure pulmonary function. It measures the volume of air exhaled by force at specific intervals following maximal inhalation. It involves having the patient breathe into and out of a mouthpiece connected to a machine or an equipped laptop, with a nose clip to ensure all airflow is directed to the mouth for proper reading. The patient is instructed to take a deep breath and breathe into the mouthpiece as hard and fast as possible. The machine can then produce two primary numbers using these results: the FVC, which is roughly the total lung capacity or volume of air exhaled in liters, and the FEV1, which is the volume exhaled in the first second. A third number is then calculated from these two preliminary numbers: the FEV1/FVC ratio, or the percentage of total lung capacity the patient can exhale in the first second. These numbers are often compared to the expected capacity/ability based on the patient’s size. The patient is tested once, then given a SABA as a bronchodilator, and the test is repeated several minutes later to assess reversibility. An improvement of 12% or 200 mL in the patient’s FEV1, or an increase of 10% of predicted FEV1, is typically considered diagnostic of asthma with variable or reversible airflow obstruction; however, an absence of this finding should not exclude the trial of a long-acting bronchodilator. In addition to diagnosis, spirometry can help determine asthma severity. Refer to Table 2, which contains severity classifications based on spirometry by the American Lung Association (ALA; Irvin, 2026; Lamb et al., 2023; Ortega & Chiarella, 2026a).
Table 2
American Lung Association (ALA) Classification of Asthma Severity
Age | Normal FEV1/FVC: | Intermittent | Mild | Moderate | Severe |
5–11 years | 8–11 years: 85% | Normal FEV1 between exacerbations FEV1 >80% predicted FEV1/FVC >85% | FEV1 >80% predicted FEV1/FVC >80% | FEV1 = 60–80% predicted FEV1/FVC = 75%–80% | FEV1 <60% predicted FEV1/FVC <75% |
12+ years | 12–19 years: 85% 20–39 years: 80% 40–59 years: 75% 60–80 years: 70% | Normal FEV1 between exacerbations FEV1 >80% predicted FEV1/FVC normal | FEV1 >80% predicted FEV1/FVC normal | FEV1 60%–80% predicted FEV1/FVC reduced 5% | FEV1 <60% predicted FEV1/FVC reduced >5% |
(ALA, 2024)
Potential barriers to primary care and pediatric providers regularly using spirometry to diagnose asthma include the time required to perform the test, the training needed to administer and interpret the results correctly, the availability of the necessary equipment, and the misconception that young children cannot perform the test correctly. Spirometry (Figure 3) can be especially helpful in ruling out differential diagnoses such as vocal cord dysfunction, functional dyspnea, anatomic obstruction, and restrictive pulmonary defects. Spirometry should be repeated at least every year or every 2 years in most patients with asthma, or more frequently if symptoms are poorly controlled. It should be avoided in patients with confirmed or suspected COVID-19 infection. For children younger than 6, alternative testing is recommended with multiple breath washout, impulse oscillometry, electrical impedance tomography, or structured light plethysmography (GINA, 2025b; NHLBI, 2020a; Perrem et al., 2024; Rosen & Colin, 2025).
Figure 3
Spirometry
(NHLBI, 2013b)
A peak flow meter (refer to Figure 4) is a small, handheld device that all patients with asthma should be given for regular home monitoring. Patients should be instructed to stand, take a deep breath, ensure the indicator is at the bottom of the device, and blow into the device as hard and fast as possible to obtain a score or PEF number. This can be repeated immediately two additional times, using the highest score from the three attempts. This should be done at a consistent time, typically first thing in the morning before any medications. Immediately after diagnosis, the patient should do this twice daily (in the morning and around lunchtime) and record the numbers for 2-3 weeks. The highest number of the 28 readings from this period will become their personal best (PB). The patient’s PB then serves as a benchmark for future monitoring, indicating a concerning change or decline in lung function. The same procedure may be repeated later during any 2- to 3-week period to reassess and update the patient’s PB. Their asthma action plan (AAP), a written instruction sheet or road map for patients with asthma to adjust medications and manage their asthma symptoms at home, is based on this PB number. A patient’s PEF number will often start to decrease before an exacerbation, before the patient even identifies any noticeable symptoms, serving as their initial warning sign. A record of highly variable PEF readings and reversibility 10–15 minutes after taking a SABA inhaler may be used as a diagnostic test for asthma if necessary in patients unable to perform spirometry successfully (Irvin, 2026; NHLBI, 2024). GINA recommends that patients also check their PEF following an exacerbation to monitor recovery, following any medication changes, if they feel an increase in their symptoms, and to help identify and pinpoint domestic or occupational triggers. They recommend regular PEF monitoring in patients with a poor perception of airflow limitation, a history of sudden and severe exacerbation(s), or severe or difficult-to-control asthma (GINA, 2025b).
Figure 4
Peak Expiratory Flow Meter

(NHLBI, 2013a)
A bronchial challenge test involves provoking symptoms by first testing spirometry, then exposing the patient to a chemical irritant such as methacholine (Provocholine), and finally retesting spirometry. The purpose is to determine if exposure causes a decrease in the patient’s FEV1. A bronchial challenge is considered positive if the FEV1 decreases by 20% from baseline after exposure to methacholine (Provocholine); this may require several exposures at progressively increasing doses. Methacholine (Provocholine) commonly causes wheezing and SOB in patients with asthma, and histamine will cause increased mucus production and bronchoconstriction. Exercise or eucapnic voluntary hyperventilation using ambient or cold temperature air can also be used for a bronchoprovocation challenge. This test is useful when airway hyperreactivity is suspected despite normal spirometry (GINA, 2025b; Sayeedi et al., 2025; Wood, 2024).
FeNO tests the fractional concentration of exhaled nitric oxide. According to GINA, it has not yet been established whether it rules in or rules out asthma. This is because, although FeNO typically increases in patients with asthma, characterized by Th2 inflammation, it also increases in nonasthma conditions such as eosinophilic bronchitis, atopy, allergic rhinitis, and eczema. It is also not elevated in certain types of asthma, including neutrophilic asthma. FeNO results are often decreased in smokers, during bronchoconstriction, or in the early phases of an allergic response (GINA, 2025b).
While preparing the EPR-4 update, the NAEPP conducted a systematic review of the evidence regarding the utility of FeNO in diagnosing and managing asthma. They found that the diagnostic utility of FeNO varies by patient and is most helpful in nonsmokers, pediatric patients, and steroid-naïve patients. Sensitivity and specificity varied with the diagnostic cutoff used. For example, in patients aged 5 and up, if a cutoff score of 20 parts per billion (ppb) or less was used, the sensitivity was 0.79 and the specificity was 0.72; if a cutoff score of 40 ppb or greater was used, the sensitivity decreased to 0.41, yet the specificity increased to 0.94. There is insufficient evidence to support the utility of FeNO in predicting asthma in patients aged 0–4 years with chronic wheezing. Regarding utility in asthma management, the NAEPP found only a weak association between FeNO results and asthma control or the risk of asthma exacerbation. However, this association was admittedly stronger in patients with atopy. They found no association between FeNO results and asthma severity. Overall, the results were poorly reproducible. The studies showed that using management algorithms incorporating FeNO results reduced the risk of exacerbations but did not affect the risk of hospitalization, QOL, asthma control, or FEV1. The NAEPP found evidence that FeNO results may help identify patients with asthma more likely to respond to ICS and may help predict impending exacerbations in patients undergoing ICS reduction or withdrawal, but not as a stand-alone test. The clinical context clues improve this predictive ability. Medications can alter FeNO results. Specifically, FeNO levels are often lower in patients taking an ICS, an LTRA, or omalizumab (Xolair), but not in those taking a long-acting beta-agonist (LABA). Further research has shown that FeNO testing is most useful when used in conjunction with other lung function tests (Ali et al., 2023; Wang et al., 2017).
The role of FeNO in the diagnosis of asthma is still evolving. The updated EPR-4 guidelines recommend using FeNO in children over 5 when the diagnosis of asthma is inconclusive after a thorough history, physical examination, and spirometry testing with bronchodilator responsiveness (or when spirometry testing cannot be performed). When FeNO results are elevated (greater than 50 ppb in adolescents and adults or greater than 35 ppb in children ages 5-12), the likelihood that the individual has asthma increases by 2.8–7.0 times. However, when reviewing FeNO test results, it is crucial to consider that allergic rhinitis and atopy can increase FeNO levels in patients with or without asthma. The EPR-4 guidelines do not recommend using FeNO in children under 5 years, as its diagnostic accuracy has not been validated in the literature (NHLBI, 2020a).
Assessing for potential differential diagnoses is extremely important when diagnosing asthma, as many respiratory and cardiac conditions often mimic asthma symptoms. For example, COPD in patients over 65 and late-onset asthma may be tough to differentiate, as they will often both respond to certain medications and have similar symptom presentations. Clues that the patient may be developing COPD instead of asthma include a history of smoking or occupational exposure and the pattern of symptom presentation. In contrast, indications that asthma is more likely include nasal polyps or steroid dependency. The most crucial resource in the case of diagnostic uncertainty is a referral to a specialist for confirmation. Table 3 outlines common differential diagnoses by age (GINA, 2025b).
Table 3
Differential Diagnoses of Asthma with Common Presenting Symptoms by Age
Any age:
Age 6–11:
Age 12–39:
Age 40+:
|
(GINA, 2025b)
Nonpharmacological Treatment of Asthma
Asthma management has three components: nonpharmacological treatment, control medications, and reliever medications. The GINA guidelines emphasize a comprehensive list of treatments patients with asthma should be educated about. They recommend smoking cessation (if the patient smokes) or avoiding environmental exposure to secondhand smoke. Patients are also encouraged to engage in regular physical activity, regardless of whether they have exercise-induced symptoms. To prevent exercise-induced bronchoconstriction (EIB), the patient should be educated on prevention techniques such as completing a warm-up before strenuous activity, using a SABA, ICS-SABA, or low-dose ICS-formoterol (Symbicort, Dulera) before exercise, or wearing a mask or scarf if symptoms are cold-induced. Physical activity is associated with improved symptom control, cardiopulmonary function, and QOL. Another reason physical activity is important is that obesity has been shown to make asthma control more difficult to achieve. Patients who are obese should be strongly encouraged to attempt a comprehensive weight loss plan. All patients with asthma should be educated on the importance of a balanced diet to maintain a healthy weight (GINA, 2025b).
Certain medications can cause worsening asthma symptoms, such as nonselective beta-blockers, NSAIDs, and angiotensin-converting enzyme (ACE) inhibitors. If cardioselective beta-blockers are indicated for treating or preventing coronary events, comorbid asthma is not an absolute contraindication, but the potential benefits versus risks must be weighed. NSAIDs should always be avoided in patients with aspirin-exacerbated asthma, although cyclooxygenase-2 (COX-2) inhibitors and acetaminophen (Tylenol) are usually well-tolerated (GINA, 2025b).
Breathing exercises may be used with pharmacological treatment to improve symptoms and QOL. The ALA has helpful patient education videos on its website regarding pursed-lip and diaphragmatic breathing. Pursed-lip breathing involves breathing in through the nose and then out very slowly through pursed lips, making sure that the exhale lasts at least twice as long as the time spent inhaling. Diaphragmatic breathing (also known as belly breathing), instructs the patient to breathe in through the nose while placing their hands or another object on their belly to reinforce filling the lungs by pulling down and out with the diaphragm into the abdomen, and then slowly exhaling, again taking two to three times the amount of time to exhale as the time spent on inhaling. Although these techniques can be helpful, they have not consistently improved lung function or decreased exacerbations (ALA, 2026a; GINA, 2025b).
Decreasing stress has been shown to enhance asthma control and lung function beneficially. Patients with asthma should be educated on which stress-relief activity or program best fits their lifestyle and personality. There is insufficient evidence that one technique is more beneficial than another. Anxiety and depression may also lead to worse asthma control, poor adherence, and decreased QOL if not appropriately treated. Patients with symptoms of anxiety or depression affecting asthma control should be referred to a mental health specialist for treatment. GINA also recommends that all patients with asthma review their vaccination records and ensure all recommended vaccinations are up to date, especially influenza and COVID-19. Insufficient evidence supports the routine use of pneumococcal and pertussis vaccinations in adults with asthma (GINA, 2025b).
The GINA guidelines previously suggested that patients with asthma avoid exposure to known triggers when possible, but now state that this is not a generally recommended strategy except for cases with mold in homes and for children with house dust mites or pets. The guidelines also recommend the avoidance of occupational allergens. Occupational asthma refers to patients who are triggered by chemical or environmental exposures during their regular workday and whose symptoms generally worsen over time. The primary goal of treatment is to limit exposure. Although many patients with asthma may not feel comfortable making drastic decisions such as changing their profession, switching schools, or moving to a rural area with less smog and air pollution, if allergen triggers are identified, they can at least engage in a program to reduce exposure to indoor allergens in their own homes and schools (GINA, 2025b).
An evidence summary conducted in preparation for the EPR-4 found a paucity of high-quality studies on the effectiveness of managing indoor allergen exposure and its effects on asthma morbidity and control. Studies that incorporate high-efficiency particulate air (HEPA) vacuum cleaners appear to reduce exacerbation rates and improve patients’ reported QOL. Mattress covers designed to reduce allergens improve nonvalidated measures of respiratory symptoms when combined with other interventions but have no clinical effect when tested independently. Consistent pest control service reduces the number of asthma exacerbations (US Department of Health and Human Services [HHS], 2020; Kalayci et al., 2022). For pediatric patients who spend a large portion of their waking hours in a school environment, Maciag and Phipatanakul conducted a systematic review of multiple randomized controlled trials to evaluate exposure to environmental allergens and the effectiveness of mitigating interventions. Unfortunately, some exposure to allergens is unavoidable, such as pet allergens brought into school on other students’ clothing or belongings. Mouse allergen proteins are also a problem in schools. One study in the review found that 98% of inner-city schools in the northeast United States contained detectable amounts of mouse allergen. Exposure to mouse allergen in schools has been associated with an increased likelihood of asthma symptom days and a 4% decrease in FEV1. The method to decrease mouse allergens is integrated pest management (IPM). Following IPM, studies showed a 75% reduction in mouse allergen correlated to increased lung growth in children. The presence of the cockroach allergens Bla g 1 and Bla g 2 is associated with decreased lung function and increased emergency room visits and hospitalizations in patients with asthma. The most effective intervention to remove cockroach allergens is IPM, which can reduce exposure risk by 90%; however, studies examining the impact of cockroach allergen reduction on asthma symptoms are mixed (GINA, 2025b; Maciag & Phipatanakul, 2022).
The NAEPPCC last published guidelines, the EPR-3, in 2007. In 2018, the National Heart, Lung, and Blood Advisory Council (NHLBAC) and NAEPPCC established a group to update these guidelines to EPR-4. In 2020, focused updates were released, concentrating on 19 recommendations addressing six topic areas. The NHLBAC also recommended that another 11 topics be acknowledged in the update, but no new recommendations were developed. One such topic was the definitions associated with asthma severity. Still in use, the EPR-3 guidelines outline severity by age range (0–4 years, 5–11 years, and 12+ years) and classify severity as intermittent and mild, moderate, or severe persistent based on impairment and risk (refer to Table 4, NHLBI, 2007). The previous category of mild intermittent was removed due to the potential for severe exacerbations even with intermittent asthma. The 2025 GINA update addressed severity, stating that it is a retrospective concept based on how difficult the person’s asthma is to treat, as assessed by symptom control and exacerbation after at least 3 months of treatment. Mild asthma is defined as well-controlled with low-intensity treatment; moderate is well-controlled with step 3 or 4 treatment; and severe is asthma that is uncontrolled despite optimal, high-intensity treatment. Once assessed, these levels correspond with a stepwise treatment algorithm outlined in the EPR-4 update and 2025 GINA updates. Step 1 refers to managing intermittent asthma, while steps 2–6 refer to persistent asthma ranging from mild to severe in ascending order. Each step has preferred and alternative treatment options based on patient presentation and preferences (GINA, 2025a, 2025b; NHLBI, 2007, 2020a).
Table 4
Asthma Severity Classification by Age
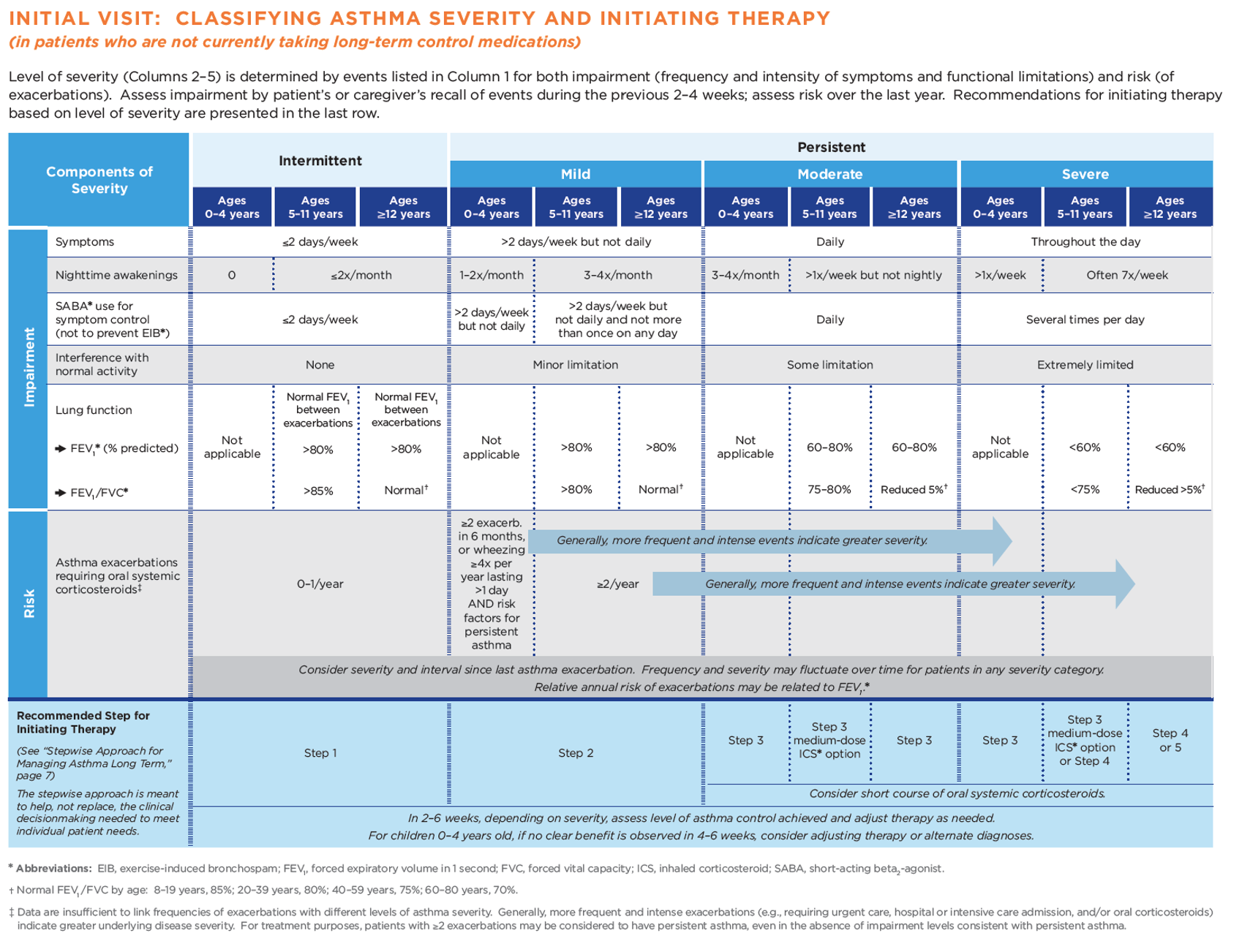
(NHLBI, 2012, p.5)
Once assessed, these severity levels correspond with a stepwise treatment algorithm outlined in the 2020 Asthma Management Guidelines and GINA updates. Step 1 refers to managing intermittent asthma, while steps 2-6 refer to persistent asthma ranging from mild to severe in ascending order. Each step has preferred and alternative treatment options based on patient presentation and preferences (GINA, 2023; NHLBI, 2020).
Immunotherapy
Immunotherapy for treating allergic asthma has become more commonplace and better studied in recent years. GINA guidelines (2025b) list immunotherapy among the recommended adjunct nonpharmacological treatments to consider for patients with stable, but not well-controlled asthma who demonstrate significant aeroallergen sensitization. There are two approaches to immunotherapy: subcutaneous immunotherapy (SCIT) and sublingual immunotherapy (SLIT). SCIT involves identifying allergens affecting the individual and then administering extracts of those allergens in progressively higher doses to induce desensitization. SCIT is associated with reduced symptoms, reduced need for medication intervention, and reduced airway hyperresponsiveness. The 2020 updates recommend using SCIT as an adjunct therapy conditionally for patients older than 5 with mild to moderate asthma that is well controlled. There are concerns regarding the design of many of the studies conducted on the effectiveness of SLIT. Despite this, SLIT is recommended in patients with asthma and allergic rhinitis related to an established house dust mite allergy who are suboptimally controlled despite ICS use and have an FEV1 of at least 70% of predicted. SLIT is not recommended in the GINA guidelines or EPR-4 updates for the treatment of allergic asthma (GINA, 2025a, 2025b; NHLBI, 2020a).
Procedural Treatment Options
Bronchial thermoplasty is a device-based treatment option that can be added at step 5 for adult patients with severe asthma that is uncontrolled despite a regimen of ICS and LABAs and a referral to a specialty asthma treatment center that either does not have access to or does not qualify for treatment with biologics. Bronchial thermoplasty is delivered via the FDA-approved Alair system, which uses heat to reduce smooth muscle inflammation in the airways. This decrease in tissue impairs the airway’s ability to constrict, allowing more airflow and easier breathing during an asthma attack. GINA guidelines caution against this treatment, as studies on its effectiveness are limited, and patients did not have their medication regimens optimized before bronchial thermoplasty. The guidelines also cite a significant placebo effect and a transient increase in asthma exacerbations during the 3-month treatment period, followed by a subsequent reduction in exacerbations following treatment. They cited no impact on lung function testing or asthma symptoms compared with sham procedures. GINA guidelines recommend that bronchial thermoplasty be performed only in adults in an Institutional Review Board-approved clinical study until more information is available on the overall effectiveness of the procedure (GINA, 2025b; Sharma & Carr, 2026). Chupp and colleagues completed a study to determine the 5-year efficacy of bronchial thermoplasty on adult patients with severe asthma. A total of 284 subjects aged 18–65 were included in the study, of whom 227 completed the 5-year follow-up. The researchers compared results 5 years posttreatment with those 12 months before treatment. They found that the number of individuals who experienced severe exacerbations decreased from 77.8% to 42.2%, emergency room visits decreased from 29.4% to 7.9%, and hospitalizations decreased from 16.1% to 4.8%. The percentage of participants taking oral maintenance corticosteroids also improved from 19.4% to 9.7% (Chupp et al., 2021).
Integration of Care
Asthma is best treated in an integrated, multidisciplinary manner. The School-Based Allergy, Asthma, and Anaphylaxis Management Program (SAMPRO) is designed by the American Academy of Allergy, Asthma, and Immunology (AAAAI) to assist students and their families in managing asthma consistently at home and at school (AAAAI, 2025). It involves four components:
- circle of support—this support and communication network includes the child, the provider, the family, the school registered nurse, and the community
- asthma management plan—this includes an AAP (medical authorization for self-carry and administration of asthma medications as needed, parental release of information) in combination with a generic asthma emergency treatment plan, which is an emergency plan for all students in the school, including stock albuterol and a way to administer the medication
- a comprehensive education plan for all school personnel
- assessment of the school environment with remediation of any triggers present (AAAAI, 2025)
In 2019, with bipartisan support from Congress and other organizations, the AAAAI initiated the School-Based Allergies and Asthma Management Program Act (HR 2468). On January 5, 2021, this Act became law to improve the safety of children with allergies and asthma while in the school setting. The Act requires that the HHS award grants to states that ensure that a school nurse or other trained professional is on the school premises and available and that children with allergies or asthma are identified and have an individualized action plan (Allergy & Asthma Network, 2025a).
Asthma Action Plan
A crucial component of comprehensive care, an AAP is a patient’s daily roadmap for managing symptoms at home. AAPs guide patients on medication changes that can be made in response to symptom or PEF changes, as well as when to seek medical attention. AAPs use a traffic light analogy with green, yellow, and red zones. An AAP helps the patient monitor their symptoms and lung function to identify where they are in the plan (green, yellow, or red zone) and the appropriate actions based on that self-assessment. The green zone is the ideal zone where patients want to be daily. This zone is characterized by the absence of cough, wheeze, chest tightness, or SOB, and a peak flow of 80% or more of the individual’s best peak flow result. The yellow zone indicates symptoms such as cough, wheeze, chest tightness, SOB, nocturnal symptoms, impact on the ability to complete daily activities, and a peak flow of 50%–79% of the individual’s best peak flow. When in the yellow zone, medication administration or adjustment is needed based on the individual action plan. The red zone indicates an asthma exacerbation or flare-up, which usually requires immediate medical intervention. Symptoms include feeling SOB with difficulty walking and talking, an inability to perform daily activities, signs of cyanosis with discoloration to the lips or fingertips, and a peak flow of less than 50% of the individual’s best peak flow result. The red zone also indicates a lack of improvement after administering quick-relief medications, or symptoms are the same or worsening after 24 hours in the yellow zone. It is recommended that all patients with asthma, regardless of age, be given a written or electronic AAP that is reviewed and, if needed, edited or updated at each follow-up visit. It is also vital for school-aged children to incorporate the AAP into the school’s asthma management program and planning, as it outlines the best practices for each student with asthma enrolled (ALA, 2026b; GINA, 2025b; NHLBI, 2021). Refer to Figure 5 for a sample AAP from the NHLBI.
Figure 5
Sample Asthma Action Plan
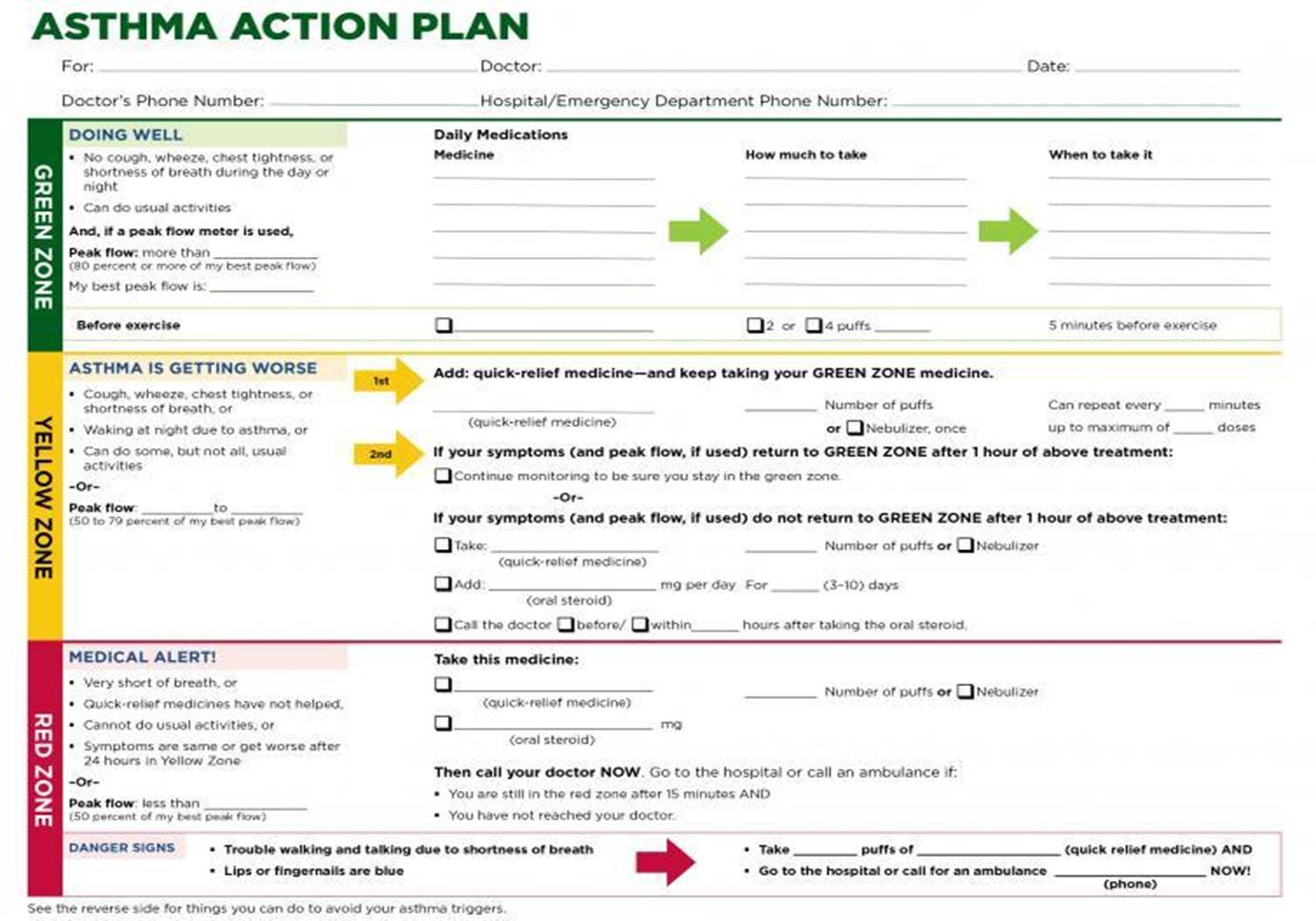
(NHLBI, 2021)
Treatment Guidelines
The extensive pharmacological management options available to patients with asthma can overwhelm providers. Options include control medications, typically taken daily on a scheduled basis regardless of symptoms. ICS, LABAs, LTRAs, long-acting muscarinic antagonists (LAMA), theophylline (Theo-24, a bronchodilator in pill form), and cromolyn sodium (Intal, a mast cell stabilizer) are control medications. For severe asthma, five biologics and one biosimilar are approved by the FDA. Reliever, quick-relief, or rescue medications work quickly to diminish symptoms, but most have a very short half-life. These include SABAs such as albuterol (ProAir, Ventolin) and terbutaline (Bricanyl, Marex; not currently available as an inhaler in the United States), or short-acting muscarinic antagonists (SAMA) such as ipratropium bromide (Atrovent). Formoterol fumarate (Symbicort, Dulera) is a longer acting but rapid-onset LABA also used as a reliever (Sharma & Chakraborty, 2023).
As previously discussed, the NAEPP last published full guidelines in 2007, with more recent updates in 2020. The original NAEPP guidelines included a practical algorithm to assess asthma severity at initial diagnosis based on symptom frequency, nighttime awakenings, SABA use, and exacerbations, in combination with everyday impairment and spirometry results, broken down by age group. The GINA 2025 update recommends a retrospective evaluation several months after treatment initiation of how difficult it is to treat the patient’s asthma. Once assessed, these severity levels correspond to the updated EPR stepwise treatment algorithm in Table 5, which assists providers in determining the best medication regimen for their patient (GINA, 2025b; NHLBI, 2020b).
Table 5
NAEPP 2020 Asthma Treatment Algorithm
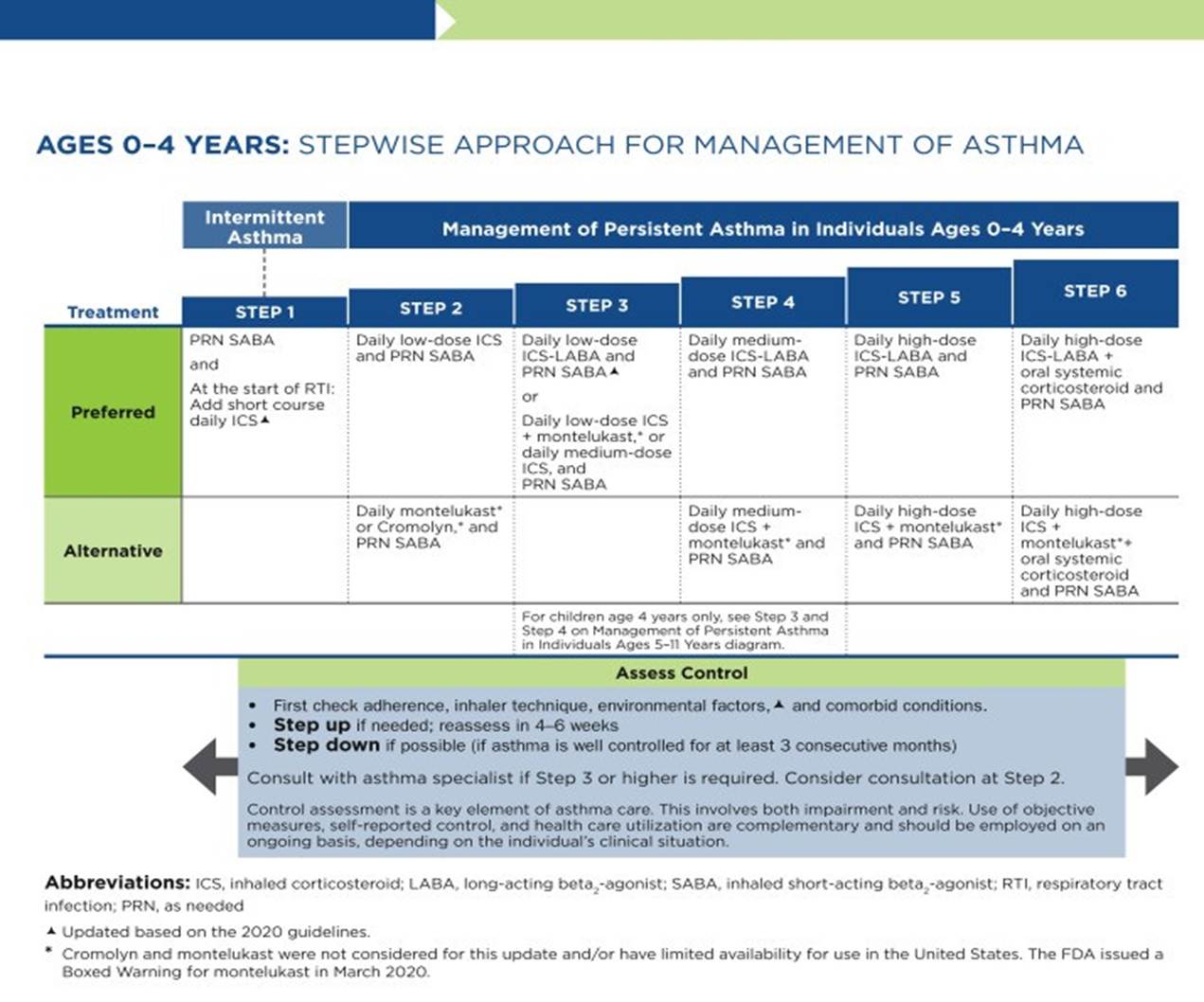
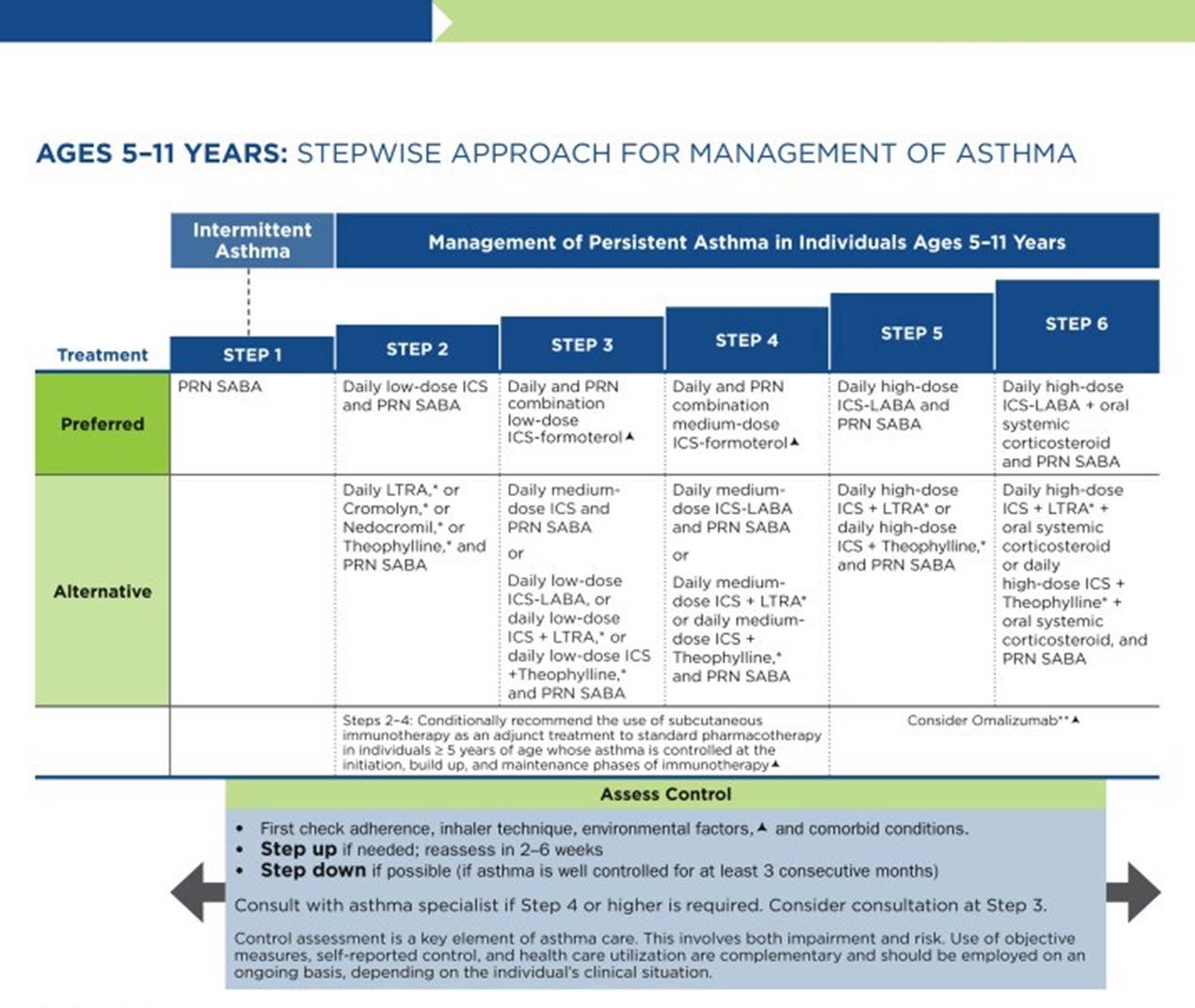
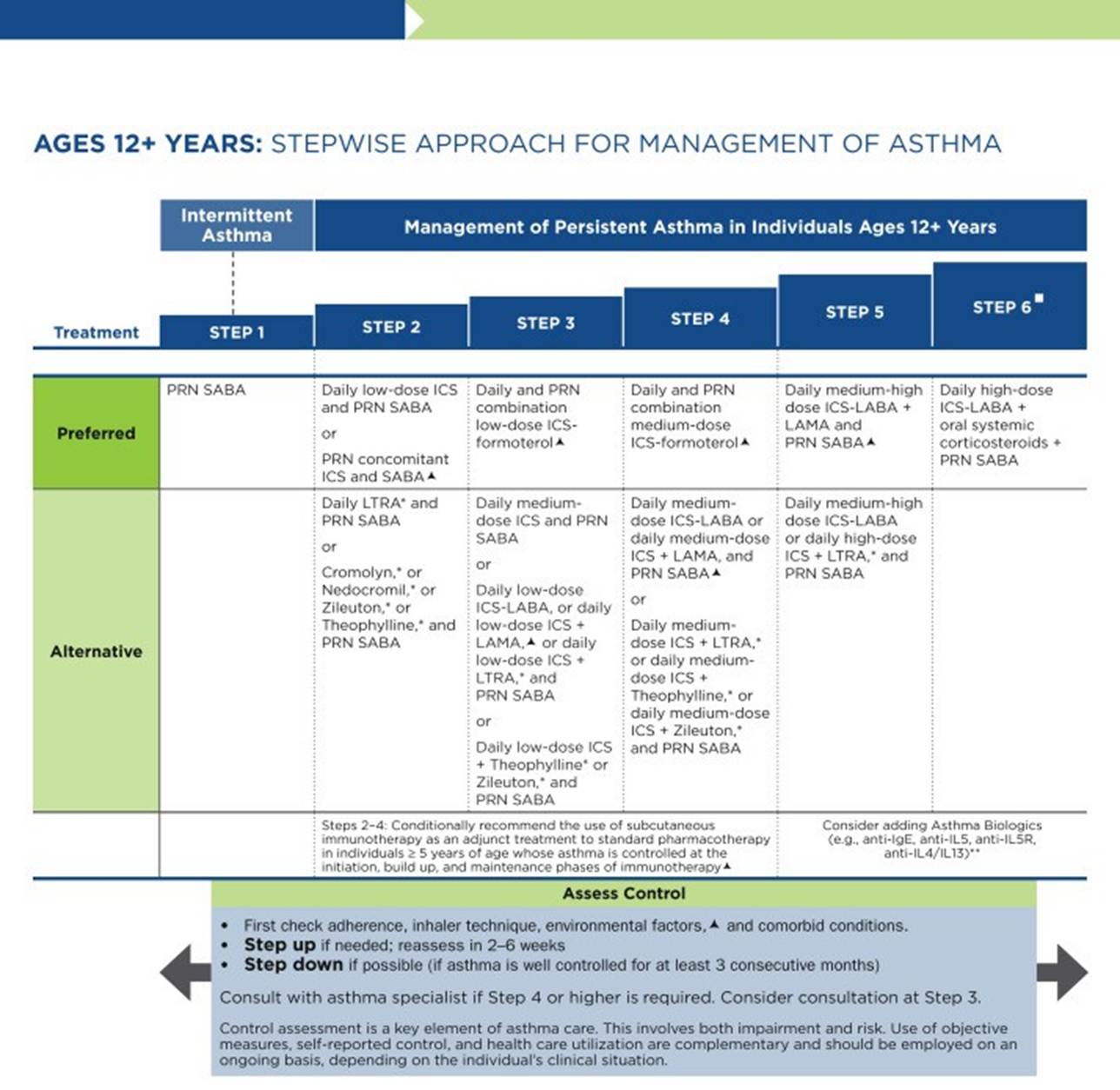
(NHLBI, 2020b)
GINA (2025b) guidelines also include a stepwise treatment algorithm similar to the EPR-4 2020 updates (refer to Table 4). The primary difference between the two is that GINA’s algorithm has just five steps. However, they specify dosage differences based on age. Similar to the NAEPP guidelines, which include preferred and alternative therapies, GINA has a two-track algorithm. Track 1 is the preferred, recommended track that includes ICS-formoterol as maintenance and reliever therapy (MART). However, alternative options are provided in Track 2 for those who cannot afford the combination MART therapy or prefer a separate control and reliever medication. Previously, the GINA guidelines did not include a stepwise treatment algorithm for children under 6 years of age, but the 2025 update added one for children 5 years of age and younger. Other major changes include how biomarkers should be used for the diagnosis, assessment, and management of asthma; updated risk factors for adolescents and adults; how extreme weather can affect people with asthma; and the management of severe exacerbations across all ages, with an updated decision tree. Both groups recommend stepping down treatment after 3 months of good control or stepping up treatment for continued symptoms/exacerbations. They both point out the importance of confirming the use of the correct inhaler technique and medication adherence, as well as treating comorbidities such as GERD, obesity, or smoking before stepping up treatment, as all of these conditions may worsen or mask asthma symptoms and lead to inappropriate treatment (GINA, 2025a, 2025b; NHLBI, 2020a, 2020b).
The first step of the EPR-4 indicates using a SABA as needed for symptom management for all age groups. The severity of symptoms guides treatment intensity, but SABAs may be administered every 20 minutes up to three times. If intermittent SABA is required more than 2 days per week, a step-up in treatment is indicated (NHLBI, 2020a).
Step 2 of the EPR-4 includes preferred and alternative treatments. For all patients, regardless of age, the preferred treatment is the addition of a low-dose ICS administered daily. The alternative treatment for those of ages 0–4 is the addition of daily montelukast (Singulair) or Cromolyn. The alternative treatment for those of ages 5 and older includes adding a daily dose of an LTRA, cromolyn sodium (Intal), nedocromil (Tilade), or theophylline (Theo-24). Another alternative option for those of ages 12 and older is zileuton (Zyflo; NHLBI, 2020a). Step two of the GINA guidelines for children of ages 6–11 includes using a daily low-dose ICS. Other controller medications that can be used but are not preferred include daily LTRA or using a low-dose ICS whenever a SABA is used. For those of ages 12 and older, the preferred treatment in step 2 is the same as in step 1: low-dose ICS-formoterol (Symbicort, Dulera) as needed. The alternative therapy is daily low-dose ICS with an as-needed SABA as a reliever medication (GINA, 2025b; NHLBI, 2020a).
Step 3 of the EPR-4 for those of ages 0–3 includes increasing the daily ICS dose to a medium dose. If an escalation to step 4 is indicated, the preferred treatment is adding an LABA. The alternative treatment in step 4 involves adding montelukast (Singulair). For children aged 4–11, steps 3 and 4 should be followed. Therefore, step 3 therapy for those of ages 4 and up is a low-dose daily and as-needed dose of ICS-formoterol (Symbicort, Dulera). For steps 3 and 4, the preferred quick-relief treatment for children 4–11 is ICS-formoterol (Symbicort, Dulera) one to two puffs as needed, up to a daily maximum of 8 puffs (36 mcg) or 12 puffs (54 mcg) for those 12 and up. Alternatives for step 3 include a medium dose of ICS with an as-needed SABA, a low-dose ICS-LABA daily, or a low-dose ICS daily plus an LTRA or theophylline (Theo-24) with an as-needed SABA. Step 4 calls for a daily medium dose of ICS-formoterol (Symbicort, Dulera), with an alternative of daily medium-dose ICS with an LABA, LTRA, or theophylline (Theo-24) plus an as-needed SABA. Step 5 treatment is based on daily high-dose ICS-LABA with a PRN SABA, while step 6 involves the addition of a systemic steroid. Alternatives include using an LTRA or theophylline instead of the LABA (NHLBI, 2020a).
The primary therapies for Steps 3 and 4 in those over 12 mirror those for 4- to 11-year-olds, but the alternatives vary somewhat. Alternative step 3 treatments include a daily low-dose ICS plus LAMA or zileuton (Zyflo) and a SABA as needed. If a step-up to step 4 is required for a patient 12+, the ICS-formoterol (Symbicort, Dulera) dose increases from a low to a medium dose in both the preferred and alternative treatment guidelines. Step 5 treatment is based on daily medium-high-dose ICS-LABA plus LAMA with a PRN SABA, while step 6 involves the addition of a systemic steroid. Alternatives include using an LTRA instead of the LABA (NHLBI, 2020a).
Intermittent ICS dosing is defined as varying in dose, frequency, or duration of administration, such as initiating a temporary course of ICS or temporarily increasing the dose. For the 2020 EPR-4 update, an executive summary regarding intermittent ICS and LAMA use was published by Sobieraj and colleagues (2018b), discussing the efficacy of intermittent ICS use by age group. They reviewed 54 randomized controlled trials and two observational studies as part of their process. In patients aged 4 and under with recurrent wheezing, intermittent ICS use with SABA (vs. SABA alone) reduced the risk of exacerbations requiring oral steroids (moderate strength of evidence) and improved QOL (low strength of evidence). In these patients, intermittent ICS reduced the risk of exacerbation requiring oral steroids, hospitalization, or rescue medication use versus regularly scheduled ICS controller use. There was insufficient evidence regarding intermittent ICS use versus nonpharmacological or no therapy in this age group. In patients aged 5–11 with persistent asthma, intermittent ICS use did not affect QOL or rescue medication use compared with ICS controller use, with low strength of evidence; insufficient evidence was available to assess the effect on other outcomes in this age group. In patients aged 12 and older with persistent asthma, intermittent ICS dosing, either alone or with ICS controller dosing, did not affect the risk of exacerbation compared with ICS controller dosing alone, with low strength of evidence. However, using intermittent and controller ICS versus controller dosing alone decreased the number of asthma-related outpatient visits based on low strength of evidence. Further research has validated these findings in adolescents and adults (Beasley et al., 2023; Cardet et al., 2023; NHLBI, 2020a; Sobieraj et al., 2018b).
Controller Medications
Inhaled Corticosteroids
ICS are the primary preferred controller medications used in both algorithms for persistent asthma. They reduce bronchial inflammation, prevent exacerbations, and often relieve cough. The onset of action is slow and gradual; therefore, the maximum benefit may take several days to weeks to be evident. Standard ICS dosing ranges vary by patient age, the guideline followed, and the specific step within the guidelines (GINA, 2025b; Liang & Chao, 2023; NHLBI, 2024). The standard low, medium, and high doses of ICS for the GINA and EPR-4 updated guidelines are outlined in Tables 6 and 7.
Table 6
Low, Medium, and High Doses of Inhaled Corticosteroids by Age per GINA
Low dose (mcg/day) | Medium dose (mcg/day) | High dose (mcg/day) | |
Adults/Adolescents (age 12 and older) | |||
Beclometasone dipropionate (Beclovent) MDI, standard particle | 200-500 | >500-1,000 | >1,000 |
Beclomethasone dipropionate (Qvar) dry powdered inhaler (DPI) or MDI, extra-fine particle | 100-200 | >200-400 | >400 |
Budesonide (Pulmicort) DPI or MDI | 200-400 | >400-800 | >800 |
Ciclesonide (Alvesco) MDI | 80-160 | >160-320 | >320 |
Fluticasone furoate (Arnuity Ellipta) DPI | 100 | 200 | |
Fluticasone propionate (Flovent) MDI or DPI | 100-250 | >250-500 | >500 |
Mometasone (Asmanex) MDI | 200-400 | >400 | |
Children (age 6-11) | |||
Beclomethasone dipropionate (Beclovent) MDI, standard particle | 100-200 | >200-400 | >400 |
Beclomethasone dipropionate (Qvar) MDI, extra-fine particle | 50-100 | >100-200 | >200 |
Budesonide (Pulmicort) DPI or MDI | 100-200 | >200-400 | >400 |
Budesonide (Pulmicort) nebules | 250-500 | >500-1,000 | >1,000 |
Ciclesonide (Alvesco) MDI | 80 | >80-160 | >160 |
Fluticasone furoate (Arnuity Ellipta) DPI | 50 | NA | |
Fluticasone propionate (Flovent) MDI or DPI | 50-100 | >100-200 | >200 |
Mometasone furoate (Asmanex) MDI | 100 | 200 | |
(GINA, 2025b)
Table 7
Low, Medium, and High Doses of Inhaled Corticosteroids by Age per NHLBI
Medication | Low dose per day | Medium dose per day | High dose per day |
Adults/Adolescents (age 12 and older) | |||
Beclomethasone dipropionate (Beclovent) MDI | 80-240 mcg | >240-480 mcg | >480 mcg |
Budesonide (Pulmicort) DPI | 180-540 mcg | >540-1,080 mcg | >1,080 mcg |
Ciclesonide (Alvesco) MDI | 160-320 mcg | >320-640 mcg | >640 mcg |
Flunisolide (Aerobid) MDI | 320 mcg | >320-640 mcg | >640 mcg |
Fluticasone propionate (Flovent) MDI | 88-264 mcg | >264-440 mcg | >440 mcg |
Fluticasone furoate (Arnuity Ellipta) DPI | 100-300 mcg | >300-500 mcg | >500 mcg |
Mometasone (Asmanex) DPI | 110-220 mcg | >220-400 mcg | >440 mcg |
Children (age 5-11) | |||
Beclomethasone dipropionate (Beclovent) MDI | 80-160 mcg | >160-320 mcg | >320 mcg |
Budesonide (Pulmicort) DPI | 80-360 mcg | >360-720 mcg | >720 mcg |
Budesonide nebules (Pulmicort, Duoresp) | 0.5 mg | 1.0 mg | 2.0 mg |
Ciclesonide (Alvesco) MDI | 80-160 mcg | >160-320 mcg | >320 mcg |
Flunisolide (Aerobid) MDI | 160 mcg | 320-480 mcg | >480 mcg |
Fluticasone propionate (Flovent) MDI | 88-176 mcg | >176-352 mcg | >352 mcg |
Fluticasone furoate (Arnuity Ellipta) DPI | 100-200 mcg | >200-400 mcg | >400 mcg |
Mometasone (Asmanex) DPI | 110 mcg | 220-440 mcg | >440 mcg |
Children (age 0-4) | |||
Budesonide nebules (Pulmicort, Duoresp) | 0.25-0.5 mg | >0.5-1.0 mg | >1.0 mg |
Fluticasone propionate (Flovent) MDI | 176 mcg | >176-352 mcg | >352 mcg |
(Mammen, 2021; NHLBI, 2020a)
Since these drugs are administered via inhalation, they are delivered directly to the site of action. As a result, lower doses can be used because the first-pass metabolism is bypassed. They are traditionally dosed daily or twice daily, regardless of symptoms. Dysphonia (a hoarse or raspy voice) is a commonly experienced side effect in 50%–60% of patients. Dysphonia is reversible after ICS treatment is discontinued. Thrush is also a common side effect of ICS. This is especially true in older adults and those also taking oral steroids. However, the risk of thrush can be significantly reduced with diligent oral hygiene after medication administration and by using a spacer or chamber (refer to Figure 6), which also helps with medication delivery when using a metered-dose inhaler (MDI). In older adults, ICS may also accelerate bone mineral loss and cause skin thinning, bruising, and adrenal suppression. Adult patients who have been using ICS chronically should undergo bone density testing. ICS has also been shown to slow growth rates in children by an average of 1 cm, although this effect is neither progressive nor entirely predictable. Testing of bone density is not recommended in children; however, children taking ICS should intake adequate amounts of calcium and vitamin D (Liang & Chao, 2023; NHLBI, 2024).
Figure 6
MDI with Attached Spacer Device

(US Food and Drug Administration [FDA], 2012)
GINA guidelines recommend a lower dose of ICS earlier rather than a higher dose with more significant side effects later. With regular ICS use, an improvement in FEV1 should be observed within days and usually plateaus in roughly 2 months. PEF readings usually increase to PB level after about 2 weeks of treatment, with variability diminishing after 3 months. They also list nasal spray corticosteroids as an alternative for patients with allergic rhinitis and a proven allergy, rather than ICS. Patients with eosinophilic asthma typically require a higher dose of ICS for inflammation management, regardless of what may seem like adequate symptom control. Because inflammation can affect the entire respiratory tract, ICS alone may be insufficient in some patients. In severe asthma, systemic steroids may be added as a last resort but should be used cautiously since they carry significantly greater adverse effects (GINA, 2025b).
Long-Acting Inhaled Beta 2 Agonists
LABAs are FDA-approved only for use with an ICS (other than formoterol [Perforomist]) and not for acute symptom relief in asthma. Adding an LABA to a low-dose ICS in adult patients with asthma who are not well-controlled with low-dose ICS alone results in better control than doubling the ICS dose. However, using an LABA alone has been shown to increase the risk of exacerbation and is not recommended. They work as bronchodilators by relaxing the smooth muscles surrounding the airway by selectively stimulating beta-2 adrenergic receptors. Examples of LABAs include salmeterol (Serevent, Advair), vilanterol (Breo Ellipta), and formoterol (Perforomist). Vilanterol’s (Breo Ellipta) half-life is 16–21 hours (allowing once-daily dosing) with an onset of about 10 minutes, formoterol’s (Perforomist) half-life is 10 hours with an onset of 5 minutes or less, and salmeterol’s (Serevent, Advair) half-life is just 5.5 hours with an onset of about 15 minutes. EPR-4 recommends a maximum daily dose of 100 mcg of salmeterol (Serevent, Advair) or 54 mcg of formoterol (Perforomist). They work exceptionally well in patients experiencing significant wheezing, SOB, and nocturnal symptoms, or those patients found to be in the noneosinophilic clinical phenotype characterized by severe symptoms but minimal inflammation. Side effects include tremors, vomiting, nausea, fever, headache, cough, dry mouth, and dyspepsia (NHLBI, 2020a; Sharma & Chakraborty, 2023).
Long-Acting Inhaled Muscarinic Antagonists
Tiotropium bromide (Spiriva) is the only LAMA approved by the FDA for asthma patients aged 11 and older in the United States (although others are approved for treating COPD). It is an antagonist to muscarinic (M3) cholinergic receptors, causing bronchodilation, with a half-life of 25 hours. GINA states that in patients older than 6 years with a history of exacerbations not well controlled on low-dose ICS and LABA, the addition of tiotropium (Spiriva) can be considered at the fourth step. It has been shown to improve lung function and modestly increase the time to severe exacerbation. Dosing is two puffs of 1.25 mcg/actuation once daily. It may take 4–8 weeks to experience any improvement. The most common side effects experienced are a direct result of the anticholinergic effects of the medication and include urinary retention, dry mouth, headaches, and dizziness. Other side effects include bronchitis, sinusitis, dyspnea, back pain, cough, dyspepsia, and nausea (GINA, 2025b; Sharma & Chakraborty, 2023).
Sobieraj and colleagues (2018b) evaluated the research regarding using LAMA as part of the executive summary when preparing the updated EPR-4. They found that in patients aged 11 or older with uncontrolled persistent asthma, adding LAMA to ICS versus placebo decreased the risk of exacerbations and improved spirometry results. They also compared the combination of LAMA and ICS with doubling the ICS dose and found no significant difference. They compared adding LAMA to ICS versus adding LABA and similarly found no significant impact. Finally, they reviewed what they termed “triple treatment,” which included ICS, LABA, and LAMA. They found that adding LAMA improved FEV1 with high strength of evidence and improved asthma control scores with low to moderate strength of evidence. However, they showed no significant effect on the risk of exacerbation or hospitalization (Sobieraj et al., 2018b). Separately, a 2018 systematic review and meta-analysis of LAMA use included 15 randomized clinical trials and over 7,000 patients, including 789 aged 12–17. They found that adding LAMA to ICS versus placebo reduced the risk of exacerbation requiring systemic steroids and improved spirometry results. They found no significant difference between ICS-LABA and ICS-LAMA. Very similar to the results above, when they compared ICS-LABA with triple therapy (ICS/LABA/LAMA), they found improvements in FEV1 and QOL scores but no decrease in exacerbation risk. A 10-year cohort study by Baan and colleagues of over 66,000 individuals found that solo LAMA use without an ICS increased the risk of exacerbations. Further studies validated the use of LABAs as a third add-on therapy, or "triple treatment," but further research is recommended (Baan et al., 2021; Casale et al., 2022; Leung & Sin, 2026; Mahay et al., 2025; Marcon et al., 2025; Sobieraj et al., 2018a).
Leukotriene Receptor Antagonists
The EPR-4 and GINA guidelines both list LTRAs such as montelukast (Singulair), zafirlukast (Accolade), or zileuton (Zyflo) as alternative options for persistent asthma treatment in patients aged 5 and above. They are available as once-daily oral tablets, and montelukast (Singulair) is also available in a granule packet. Zileuton (Zyflo) also has a slightly different mechanism of action, working as a 5-lipoxygenase inhibitor to interfere with leukotriene formation, while montelukast (Singulair) and zafirlukast (Accolade) both function as selective LTRAs blocking the leukotriene portion of the inflammatory cascade (GINA, 2025b; NHLBI, 2020a; Sharma & Chakraborty, 2023).
GINA specifies that these oral medications may be an appropriate daily controller choice in patients who experience intolerable adverse effects from ICS or who have concomitant allergic rhinitis, and as an alternative in EIB. It is an alternative adjunct to ICS treatment but is less effective than adding LABA. It can also be considered an optional adjunct therapy in patients with aspirin-sensitive asthma (GINA, 2025). EPR-4 specifies that montelukast (Singulair) may be used in children as young as 1, while zafirlukast (Accolade) and zileuton (Zyflo) should not be used in patients under 5. They further specify that both zafirlukast (Accolade) and zileuton (Zyflo) require regular liver function monitoring. They also suggest LTRAs as an alternative to treating EIB (GINA, 2025b; NHLBI, 2020a).
Before prescribing these medications, providers must weigh the benefits versus the risks of adverse effects. Side effects of these medications include headaches, eczema, laryngitis, pharyngitis, dental pain, dyspepsia, cough, sinusitis, hepatitis, and allergic granulomatous angiitis (Churg-Strauss syndrome). Montelukast (Singulair) can cause neuropsychiatric events such as hostility, aggressive behavior, agitation, dream abnormalities, hallucinations, and suicidal behavior, and as of 2020, the FDA has required a black box warning for this serious mental health effect. Due to the risk of hepatoxicity, LTRAs are contraindicated in patients with hepatic dysfunction (Hartert & Bacharier, 2025; Sharma & Chakraborty, 2023).
Theophylline
Theophylline (Theo-24) is a xanthine derivative administered orally that functions by antagonizing adenosine receptors and increasing cyclic adenosine monophosphate (cAMP) and decreasing the production and release of pro-inflammatory signals, specifically TNF-alpha and leukotriene, thereby causing smooth muscle relaxation and bronchodilation. It can be beneficial for nocturnal symptoms. EPR-4 guidelines recommend theophylline (Theo-24) as an alternative to low-dose ICS in step 2 treatment, as an adjunct to ICS or ICS-LABA in steps 3, 4, and 5, or in step 6 in conjunction with ICS-LABA in an attempt to avoid a course of oral corticosteroids. It is available in liquid, capsule, or sustained-release tablet form. It is typically dosed at 10 mg/kg/day initially (NHLBI, 2020a).
GINA guidelines offer theophylline (Theo-24) as an alternative initial controller medication in adolescents and adults with initial presentation of asthma symptoms, or SABA use more than twice weekly, but note that this is typically less effective than low-dose ICS. They also mention that short-acting theophylline (Theo-24) should not be used as a reliever medication due to its poor efficacy, slower onset of action, and higher risk of adverse effects than SABAs. GINA guidelines also list theophylline (Theo-24) as an adjunct treatment option with ICS or ICS-LABA in adolescents and adults, but do not recommend its use in children (GINA, 2025). Potential side effects of theophylline (Theo-24) include headaches, insomnia, irritability, restlessness, seizures, tremors, tachycardia, cardiac arrhythmias, urinary retention, and acute myocardial infarction. Theophylline (Theo-24) may worsen GERD symptoms by relaxing the lower esophageal sphincter. Theophylline (Theo-24) also has a narrow therapeutic range and requires serum blood level monitoring at least every 6 months (GINA, 2025b; Sharma & Chakraborty, 2023).
Cromolyn sodium
Cromolyn sodium (Intal) is a mast cell stabilizer that decreases the degranulation of pro-inflammatory mediators such as histamine and leukotrienes, thereby blocking the cellular response to inhaled antigens that can trigger asthma exacerbations. Cromolyn sodium (Intal) can be administered via MDI or nebulizer; however, a significant limitation of cromolyn sodium (Intal) is the need for a nebulizer and the need to be dosed four times daily to be effective. Adverse effects vary based on the route of administration. Effects of inhalation include throat irritation, laryngeal edema, drowsiness, dizziness, bronchial irritation, cough, and hoarseness (Minutello & Gupta, 2024). Cromolyn sodium (Intal) is listed in EPR-4 as an alternative controller medication in step 2; however, insufficient research demonstrates its safety and efficacy in children under 2. It is also one of the options that may be used to pretreat EIB before exercise (NHLBI, 2020a). The updated GINA (2025b) guidelines did not mention cromolyn sodium (Intal) or other mast cell stabilizers.
Biologics
For severe asthma, there are six biologics approved by the FDA that work by diminishing or blocking the effects of various steps in the inflammatory cascade, such as omalizumab (Xolair, an antibody that binds IgE), dupilumab (Dupixent, an antibody to IL-4), mepolizumab (Nucala, an antibody to IL-5), benralizumab (Fasenra, an antibody to IL-5), reslizumab (Cinqair, an IL-5 antagonist), and tezepelumab (Tezspire, an antithymic stromal lymphopoietin [anti-TSLP]). Omalizumab (Xolair) is the only biologic recommended in the EPR-3 treatment guidelines; when the EPR-4 updates were released, biologic agents were listed as an emerging topic and were not included in the update (NHLBI, 2020a). GINA guidelines include all six biologics as optional adjunct treatments in step 5 for patients aged 6 and older with uncontrolled moderate to severe allergic asthma despite step 4 treatment. In March of 2025, the FDA approved the first asthma-related biosimilar, omalizumab (omalizumab-igec, Omylclo, Celltrion), to decrease the costs of biologics through a streamlined approval process (GINA, 2025a, 2025b; Khan et al., 2026).
Omalizumab (Xolair)
Omalizumab (Xolair) is an FDA-approved medication for moderate to severe allergic asthma in patients aged 6 and older with elevated IgE levels. It functions as a monoclonal antibody that binds IgE. Treatment with omalizumab (Xolair) may decrease the frequency of asthma exacerbations, the need for corticosteroids, and symptoms. It is delivered as a subcutaneous injection every 2–4 weeks. The dose is between 75 and 375 mg based on the patient’s weight and IgE levels before starting treatment. The manufacturer has a table and tool to calculate dosing based on individual patient values. Adverse effects of omalizumab (Xolair) include headaches, fatigue, peripheral edema, abdominal pain, leg pain, injection site reaction, myocardial infarction, and pulmonary embolism (Ortega & Chiarella, 2026b; Woods, 2023).
Dupilumab (Dupixent)
Dupilumab (Dupixent) is a monoclonal antibody targeting the IL-4-alpha subunit receptor that has been shown to significantly reduce exacerbations and improve lung function and asthma control in patients older than 6 with moderate to severe asthma with an eosinophilic phenotype or those who are oral corticosteroid-dependent. It is thought to function by inhibiting IL-4 and IL-13 activity. It is given via subcutaneous injection every 2 weeks. There are two dosing schedules. In the first, the initial dose is 400 mg, followed by 200 mg administered every other week. In the second, the initial dose is 600 mg, followed by 300 mg administered every other week. The higher dosing schedule is reserved for patients who are dependent on oral corticosteroids, to reduce their dose or eliminate their use of oral corticosteroids. Side effects include pain or redness at the injection site, sore throat, fever, dizziness, facial rash, diarrhea, toothache, insomnia, eosinophilia, and oral sores (Ortega & Chiarella, 2026b; Woods, 2023).
Mepolizumab (Nucala)
Mepolizumab (Nucala) is a humanized monoclonal antibody to IL-5 approved by the FDA for the adjunctive treatment of severe eosinophilic asthma in patients 6 years of age and older. Dosing for patients of ages 6–11 is 40 mg, and for patients 12 and older is 100 mg, and is administered via subcutaneous injection every 4 weeks. Clinical trials showed that treatment is most effective when serum eosinophil counts are above 0.15× 109/L; however, this value can be affected by long-term oral corticosteroid use. Mepolizumab (Nucala) has effectively reduced or eliminated the need for treatment with oral corticosteroids. Side effects of treatment include headaches, injection site reactions, abdominal pain, pruritus, eczema, fatigue, and hypersensitivity reactions (GINA, 2025a; Ortega & Chiarella, 2026b; Sharma & Chakraborty, 2023).
Benralizumab (Fasenra)
Benralizumab (Fasenra) is a humanized monoclonal antibody that binds to the IL-5-alpha receptor, inhibiting eosinophils’ proliferation in the bone marrow. It is an FDA-approved adjunctive therapy for patients 12 and older with severe eosinophilic asthma. It has been shown to reduce or eliminate the need for oral corticosteroids and decrease the frequency of exacerbations. The recommended dose is 30 mg administered subcutaneously every 4 weeks for 3 doses, then every 8 weeks thereafter. Potential side effects include headaches, pyrexia, pharyngitis, and hypersensitivity reactions (GINA, 2025a; Ortega & Chiarella, 2026b; Sharma & Chakraborty, 2023).
Reslizumab (Cinqair)
Reslizumab (Cinqair) is a humanized monoclonal IgG4 antibody to IL-5 that is FDA-approved as adjunctive therapy for patients over 18 with uncontrolled severe asthma with an eosinophilic phenotype. It has been shown to decrease oral corticosteroid use and the frequency of exacerbations. It is administered over 20–50 minutes via IV infusion at a dose of 3 mg/kg every 4 weeks. Possible side effects include oropharyngeal pain, myalgia, muscle spasms and fatigue, chest and neck pain, elevated creatine phosphokinase (CPK), antibody development, and anaphylaxis (GINA, 2025a; Ortega & Chiarella, 2026b; Sharma & Chakraborty, 2023).
Tezepelumab (Tezspire)
Tezepelumab (Tezspire) is a novel biologic IgG2 monoclonal antibody that blocks the effects of thymic-stromal lymphopoietin (TSLP). This cytokine is released when the epithelium is irritated by an allergen or another antigen, one step upstream from IL-4 and IL-13. It was approved by the FDA in December 2021 for use in patients 12 and older as an adjunct to treat severe, uncontrolled asthma. The recommended tezepelumab (Tezspire) dose is 210 mg, administered subcutaneously every 4 weeks. In clinical trials, the most commonly reported adverse effects included pharyngitis, arthralgia, and back pain. There is also a risk for hypersensitivity reactions (UpToDate Lexidrug, n.d.).
Azithromycin (Zithromax)
For severe asthma in adults, the GINA guidelines recommend adding azithromycin (Zithromax) 500 mg three times weekly after a specialist referral and initiation of high-dose ICS-LABA (Step 5). Before initiating azithromycin (Zithromax), the provider should obtain a sputum sample for atypical mycobacterial testing and an ECG to assess for a prolonged QT interval (this should be repeated after 1 month of treatment). When using an antibiotic such as azithromycin (Zithromax), the potential for antimicrobial resistance should be weighed against the benefits of treatment. The suggested treatment duration is 6 months, as clinical trials did not demonstrate an improvement after 3 months. The most commonly reported side effect is diarrhea (GINA, 2025a).
Quick Reliever Medications
Reliever or rescue medications are used to treat asthma exacerbations or the sudden onset of symptoms as needed. Examples of reliever medications include ICS-formoterol (Symbicort, Dulera), ICS-SABA, or SABA alone. Albuterol (Pro-Air, Ventolin) and levalbuterol (Xopenex) are bronchodilators that selectively stimulate beta-2 adrenergic receptors, like the previously mentioned LABAs, relaxing airway smooth muscles. Their half-life is 2.7–6 hours. Both are available as MDIs or nebulizer solutions, and albuterol (Pro-Air, Ventolin) is also available in oral tablets, extended-release oral tablets, or liquid syrup. Terbutaline (Bricanyl) is a SABA available in tablet form and a subcutaneous injection with a half-life of 3–4 hours. It is approved for use up to three times daily in patients aged 5 and older. EPR-4 and GINA guidelines suggest using SABAs like albuterol (Pro-Air, Ventolin) on an as-needed basis in patients with intermittent asthma. As mentioned, formoterol (Perforomist) is a quick-onset LABA with a 10-hour half-life. Ipratropium bromide (Atrovent) is a SAMA that creates bronchodilation by antagonizing acetylcholine receptors. It has a half-life of 2 hours and is available as a nebulizer solution that can be mixed with albuterol (Pro-Air, Ventolin) or levalbuterol (Xopenex), or as an MDI that can be used independently. Both guidelines suggest utilizing the patient’s report of reliever use frequency to help gauge the level of symptom control in patients with asthma (GINA, 2025b; NHLBI, 2020a; Sharma & Chakraborty, 2023).
MART/SMART
In the GINA treatment guidelines (2025b), low-dose ICS-formoterol (Symbicort, Dulera) is listed in steps 3–5 as an option for controller and reliever medication. This is known as MART and can only be used with ICS-formoterol inhalers, such as budesonide-formoterol (Symbicort), in patients of ages 12–17. The basic concept of MART is as follows: traditional asthma management involves one or two inhalers for daily control/maintenance, with a separate reliever inhaler used as needed. Alternatively, the MART method instructs patients to utilize one inhaler, a combination of ICS and formoterol, a rapid-onset LABA, for maintenance and as-needed symptom control. Some also refer to MART as single-inhaler maintenance and reliever therapy (SMART); the GINA guidelines use the term MART, whereas the NAEPP guidelines use SMART. MART is also the preferred treatment method in steps 3 and 4 for children of ages 6–11. Studies have shown that the use of MART with low-dose ICS-formoterol reduces severe exacerbations and provides a similar level of control compared to ICS-LABA or a higher dose of ICS as maintenance medication in combination with a SABA as needed (Evidence level A indicating a large amount of supporting data). One meta-analysis demonstrated that switching patients in step 3 with poorly controlled asthma to MART reduced severe exacerbations by 29% compared to an ICS-LABA maintenance dose plus an as-needed SABA (alternative step 4) and reduced symptoms by 30% compared to the alternative regimen of step 3. There is currently no evidence on initiating MART in patients taking biologics; however, there is no contraindication to starting a biologic in patients already using MART (GINA, 2025a, 2025b).
The NAEPP also recommends using MART (or SMART) in steps 3 and 4 for individuals aged 4–11, and in step 4 for those aged 12 and older. For individuals 5–11, the evidence supports using MART instead of an equivalent, low, or medium dose of ICS-LABA plus an as-needed SABA; however, the evidence was insufficient to make recommendations for MART compared to high-dose ICS-LABA. Three large randomized controlled trials (RCTs) involving 4,662 individuals aged 12 or older compared the use of MART versus daily ICS (budesonide) plus an as-needed SABA. The RCTs showed a reduction in the relative risk of exacerbations from 35% to 51%. These RCTs recommended the use of MART for adolescents and adults with a high certainty of evidence. Small studies have shown promising results in children, but research is lacking to support the broad use of MART in the pediatric population. To help bridge this gap, the Children’s Anti-inflammatory Reliever (CARE) trial, an RCT of 400 children aged 5–11, will assess the safety and efficacy of MART therapy compared with traditional treatment over 52 weeks. A recent meta-analysis by Slob and colleagues raises questions about how genetic variations affect asthma in children, specifically the ADRB2 Arg16 allele, for which individuals with the allele have been found to have reduced responsiveness to LABA therapy. For those affected, MART therapy with an ICS and an LABA may increase the risk for exacerbations in comparison with therapies such as increased ICS dose or an ICS-LTRA. Given these findings, to ensure safety and efficacy prior to initiating MART therapy in children, genotyping may be prudent to identify and appropriately treat those with the ADRB2 Arg16 allele. The FDA has not approved MART therapy despite research demonstrating its effectiveness in adolescents and adults. This causes barriers to use due to insurance coverage issues (AAAAI, 2024; Barry et al., 2024; Di Cicco et al., 2025; NHLBI, 2020a; Slob et al., 2025).
Per the EPR-4 expert panel, more research is needed to address this recommendation. The benefits versus risks of ICS use need to be differentiated based on race and ethnicity. There also needs to be more research on the effects on growth in children aged 0–4 who require short courses of ICS treatment for wheezing triggered by a respiratory tract infection. Validation through research is also recommended on the effectiveness of using MART compared to high doses of ICS-LABA with a SABA as needed in children of ages 4–11. Further research is also needed on the effectiveness of other rapid-onset LABAs in combination formulations used for both maintenance and reliever therapy (NHLBI, 2020a).
Assessment of Asthma Control
The key to effectively utilizing this stepwise approach is accurate and consistent assessment of symptom control at each follow-up visit. During the follow-up visit, the provider should assess symptom control and exacerbation frequency since the last visit, lung function, side effects, QOL, and overall patient satisfaction with asthma care. The patient should be asked about nighttime awakenings and daytime symptoms. Medication adherence should be discussed with nonjudgmental and open-ended statements and questions. The inhaler technique should be assessed at each visit, and the presence of an up-to-date, appropriate AAP should be confirmed. These follow-up visits should occur every 2–6 weeks while the patient is gaining control, every 1–6 months to monitor whether the patient is well-controlled, or every 3 months if a step-down in therapy is anticipated or being carried out. This follow-up should include spirometry on all patients over the age of 4 at least every year or two, as well as the use of validated symptom control tools in all patients over the age of 11, according to the NAEPP. Good control is a combination of decreased functional impairment and future exacerbation risk or damage (Hartert & Bacharier, 2025; NHLBI, 2020a).
According to GINA recommendations, follow-up visits to assess control should occur 1–3 months after the initial diagnosis, and then every 3–6 months, depending on the level of control. A follow-up is also recommended within a week of an exacerbation requiring an emergency room visit and 3–6 weeks after any medication change. In children who have experienced an exacerbation and are at risk of a repeat exacerbation, a follow-up should be completed within 1–2 days and again in 1–2 months. FEV1 should be reassessed 3–6 months after starting long-term control treatment to establish the patient’s PB, and periodically after that, but at least every year or two in asthma patients over the age of 4 (GINA, 2025b).
Asthma control is the extent to which a patient’s asthma signs and symptoms are monitored, and how impairments and the risk of adverse effects are minimized by treatment. Control is classified as well-controlled, not well-controlled, and very poorly controlled when considering symptom impairment and future risk. The overall goal of asthma treatment is to achieve good control, which is possible in most patients. Patients that have their asthma controlled do not use their quick-reliever medications for more than two days per week, do not experience nighttime awakenings more than twice per month, have their PEF or FEV1 within 20% of their PB, and have not had more than a single exacerbation requiring urgent medical treatment or the use of oral glucocorticoids within the past year (Hartert & Bacharier, 2025; Ortega & Chiarella, 2026a). Asthma control has two facets: symptom control and the risk of future adverse events or exacerbations (GINA, 2025b). Numerous screening tools can be used to assess asthma control in adolescents and adults, such as:
Simple screening tools:
- Consensus-based GINA symptom control tool—a four-question tool that asks about daytime symptoms or use of reliever medication more than twice per week, nighttime awakenings, and any activity limitation in the last 4 weeks
- Primary Care Asthma Control Screening Tool (PACS)—five simple yes/no questions regarding symptoms occurring more than once weekly for the last month
- 30-second Asthma Test—a self-report of symptoms based on five yes/no questions
Categorical symptom control tools:
- Royal College of Physicians’ Three Question Tool—a categorical tool that asks about activity limitation, daytime/daily symptoms, and difficulty sleeping in the last 30 days
- Asthma APGAR tool—includes a patient self-assessment addressing activity limitation, symptom frequency, asthma triggers, adherence to the treatment regimen, and effectiveness of treatment; one US-based study showed that utilizing the Asthma APGAR tool in primary care offices for ages 5–45 led to improved asthma control, reduced urgent medical treatment (i.e., hospitalizations), and improved adherence to treatment guidelines
- Numerical asthma control tools:
Asthma Control Questionnaire (ACQ)—a numerical self-assessment of morning symptoms, limitation in activity, nighttime awakenings, SOB, wheezing (in ACQ-5), use of reliever medication (in ACQ-6), and prebronchodilator FEV1 (in ACQ-7); final score ranges 0–6, <0.75 is well controlled, 0.75–1.5 yellow/gray zone, >1.5 is poorly controlled; may be used in adults and pediatrics; GINA prefers the use of the ACQ-5 since the question addressing reliever use does not differentiate between regular and as-needed use
Asthma Control Test (ACT)—a numerical test that includes a patient report of the level of control, limitation in activity, nighttime awakenings, SOB, and use of reliever medication; scores range from 5–25; 20–25 is well-controlled, 16–19 not well controlled, <16 very poor control; childhood ACT (c-ACT) is available with separate sections for the child and guardian to complete
Other tools designated for use in children aged 4 and over include:
- Test for Respiratory and Asthma Control in Kids (TRACK)—for use in pediatrics, includes a recent history of exacerbations
- Composite Asthma Severity Index (CASI)—for use in pediatrics, includes a recent history of exacerbations (GINA, 2025b)
GINA guidelines state that persistent bronchodilator reversibility of greater than 12% or 200 mL in a patient on a long-term control medication, or who was given a dose of SABA within the last 4 hours or LABA within the previous 24 hours when administered twice daily, or 36 hours when administered once daily, indicates uncontrolled asthma. Similarly, excessive variability in a patient’s PEF readings indicates suboptimal control and an increased risk for exacerbations in the future. An FEV1 less than 60% predicted is an independent predictor of future exacerbation risk and accelerated decline in lung function. This means that if a patient has a decreased FEV1 but minimal symptoms, the provider needs to consider whether the patient is significantly limiting their lifestyle to avoid symptom provocation or whether they have a poor perception of airflow limitation secondary to untreated airway inflammation. Conversely, if a patient presents with increased symptoms but good or acceptable spirometry results, the provider must consider differential diagnoses such as undetected GERD, cardiac disease, or a cough related to postnasal drip. Table 8 outlines the investigation of poorly controlled asthma despite ICS-treatment (GINA, 2025a, 2025b).
Table 8
Investigating Poor Symptom Control and/or Exacerbations Despite ICS-Containing Treatment
Observe the patient using their inhaler Discuss barriers to use and adherence | Check against inhaler checklist while observing use of inhaler. Demonstrate the correct method and recheck up to three times. Use empathy to discuss poor adherence if identified and ask about costs, refill frequencies, and beliefs. |
Confirm asthma diagnosis | If evidence of variable expiratory airflow limitation is lacking on spirometry or other lung function tests, consider cutting the ICS dose in half, repeating lung function tests in 2–3 weeks, and checking for an action plan. Consider testing for biomarkers for Type 2 asthma. |
Eliminate potential risk factors if possible Assess and treat comorbidities | Simplify regimen for adolescents and adults by moving to GINA track 1 Assess for risk factors or inducers (e.g., smoking, beta-blocker or nonsteroidal anti-inflammatory drug [NSAID] use, occupational or household allergen exposure) and manage as possible Assess for comorbid conditions that could be contributing to symptoms and exacerbations and treat (e.g., rhinitis, obesity, gastroesophageal reflux disease (GERD), depression/anxiety, obstructive sleep apnea) |
May try short-term step-up in treatment | May try 3- to 6-month (short-term) step-up to the next level of treatment or an alternative treatment option on the current level By using shared decision-making, the possible risks and benefits are balanced. |
Refer to expert | If after 3–6 months on high-dose ICS-LABA, asthma remains uncontrolled, or risk factors are ongoing, refer to expert Consider referral before 6 months for very severe or difficult to manage asthma, with doubtful diagnosis, or in cases of suspected occupational asthma |
(GINA, 2025a)
Treatment of Exacerbations
The EPR-4 updated guidelines do not address the management of asthma exacerbation. The EPR-3 guidelines (NHLBI, 2020a) suggest first assessing the severity of the exacerbation utilizing a physical exam, the patient’s report of symptoms, and signs of breathlessness or SOB (audible wheezing, retractions, accessory muscle use). In patients over 5 years of age, lung function testing, such as spirometry or a peak flow meter, may also be used to quantify the limitation in lung function, if possible. Supplemental oxygen should be used to treat any existing hypoxemia. Continuous or repeated inhaled SABA (with or without inhaled ipratropium bromide [Atrovent] if severe) should be used to reduce airflow obstruction caused by bronchoconstriction. Ipratropium bromide (Atrovent) is a SAMA that acts as a bronchodilator by antagonizing acetylcholine receptors, similar to tiotropium bromide (Spiriva), a LAMA. Systemic steroids should be started in patients with moderate to severe exacerbation or suboptimal response to SABA treatment to treat the underlying inflammation. The initial assessment should be repeated periodically to monitor treatment response. Patients who present to the ED for care or are ultimately hospitalized should be discharged with medications (SABA, oral corticosteroids, and possibly the initiation of ICS), a referral for follow-up, an asthma discharge plan, and any patient education that may apply, such as inhaler use and proper technique and environmental trigger exposure (NHLBI, 2020a). GINA guidelines list life-threatening symptoms that providers should look for in patients with asthma exacerbations, which include drowsiness, confusion, and a silent chest. They provide the following guidance on admission to the hospital versus discharge home from the ED (GINA, 2025a, 2025b):
- If pretreatment FEV1 or PEF is less than 25% of predicted or PB, or posttreatment FEV1 or PEF is less than 40% of predicted or PB, hospitalization is recommended.
- If posttreatment lung function is 40%–60% of what was predicted, a discharge may be possible after considering the patient’s risk factors and availability of follow-up care.
- If posttreatment lung function is greater than 60% of predicted or PB, discharge is recommended after considering risk factors and the availability of follow-up care.
Other factors associated with an increased likelihood of the need for admission include:
- female sex, older age, and non-White race
- use of more than eight beta 2-agonist puffs in the previous 24 hours
- the severity of the exacerbation (e.g., need for resuscitation or rapid medical intervention on arrival, respiratory rate above 22 bpm, oxygen saturation less than 95%, final PEF less than 50% of predicted)
- history of severe exacerbations (e.g., intubations, asthma admissions)
- previous unscheduled office and ED visits requiring the use of oral corticosteroids (GINA, 2025b)
In very severe exacerbations or in those patients who are not responding to the treatments mentioned above, intravenous magnesium sulfate (MgSO4) or helium-oxygen therapy (Heliox) should be considered (NHLBI, 2020a). Regarding the use of helium-oxygen therapy (Heliox), the GINA guidelines cite a systematic review comparing Heliox to air-oxygen therapy that found no benefit. The guidelines state that they discern no role for this treatment in routine care; however, it may be considered in patients who do not respond to conventional treatment. However, cost and availability are barriers to the use of this treatment modality (GINA, 2025b). The GINA guidelines indicate that randomized trials in patients with mild-moderate asthma showed no benefit from using MgSO4. However, a single 2 gm IV infusion administered to an adult over 20 minutes has been shown to reduce hospitalization rates in:
- adult patients with FEV1 less than 25%–30% of predicted at presentation
- patients with persistent hypoxemia who fail to respond to initial treatment
- pediatric patients whose FEV1 falls to less than 60% of what was predicted after 1 hour of treatment (GINA, 2025b)
Special Populations
Within asthma care, a few special populations warrant some specific treatment recommendations. Asthma affects 3%–8% of all pregnancies, making it the most common chronic condition among pregnant individuals. In the United States, 8.4%–8.8% of pregnant individuals have asthma. Asthma during pregnancy can increase the risk of preeclampsia, preterm delivery, low birth weight, or perinatal mortality by 15%–20%. Those with severe asthma have an elevated risk of the complications noted above of 30%–100%. Approximately 5.8% of pregnant individuals are hospitalized due to an asthma exacerbation, which is more common during the second trimester. This is due to hormonal and anatomical changes and cessation or reduction of asthma medications solely out of fear of fetal harm. Those with asthma should be monitored closely to ensure the fetus receives enough oxygen. Pregnancy does not always complicate asthma; one-third of individuals do not experience any change, one-third experience improvement, and one-third experience worsening symptoms. An improvement or worsening of symptoms may warrant changes in medication and treatment. Although there are concerns regarding administering any medication during pregnancy, the benefits of asthma control greatly outweigh any potential risks (Evidence level A). Most asthma medications are acceptable during pregnancy, but they recommend ICS as the preferred long-term controller. Unfortunately, there is limited data regarding the use of biologics for severe asthma control during pregnancy; however, it is recommended that pregnant individuals continue taking prescribed biologics, especially if they have been well-tolerated and effective at controlling symptoms and decreasing exacerbations. Maintenance and reliever medications should be continued during labor and delivery. Some individuals experience an asthma exacerbation during childbirth due to bronchoconstriction brought on by hyperventilation. In this case, a SABA should be administered. If high doses of SABA are needed during labor, the blood glucose levels of the infant should be monitored for the first 24 hours due to the risk of hypoglycemia, especially if the birth is considered preterm (Chambers et al., 2021; GINA, 2025b; Schatz & Weinberger, 2023; Shebl & Chakraborty, 2023).
Approximately 20% of menstruating individuals are affected by perimenstrual asthma (also called catamenial), characterized by worsening asthma control during the premenstrual phase. Risk factors include obesity, severe asthma, and older age. These individuals also tend to have dysmenorrhea, premenstrual syndrome, and shorter cycles but longer periods of active menstruation. In addition to standard asthma treatment, oral contraceptives and LTRAs may be helpful for these patients (GINA, 2025b).
Older adults are at a higher risk of medication interactions. All patients should be warned about the risk of osteopenia or osteoporosis with prolonged corticosteroid use, but older patients may be at increased risk for this complication or its sequelae. Older adults also typically experience diminishing lung function over time, increased sensitivity to medication adverse effects, and decreased medication clearance. The gradual, progressive decline in spirometry results observed in some asthma patients over their lifetime is fixed airflow limitation. It is usually incomplete and reversible with appropriate treatment. GINA guidelines recommend a streamlined regimen and easy-to-use inhalers (GINA, 2025b; NHLBI, 2024).
Adolescent patients will experience frequent changes in symptoms, control, and therapy needs due to their rapid growth and hormonal changes during this stage of life. Cognitive and social changes may also occur, influencing asthma management. Adolescent patients should be assessed separately from their caregivers, at least briefly, to ask about smoking, as smoking rates are higher among adolescents diagnosed with chronic conditions than healthy ones (GINA, 2025b).
Those diagnosed with EIB typically experience worsening symptoms following the cessation of physical activity. There is strong evidence that ICS treatment significantly reduces the incidence of EIB. There is also strong evidence that premedication with a SABA, LABA, or chromones before engaging in physical activity prevents EIB; however, tolerance to SABAs and LABAs has developed with regular (more often than once daily) use (GINA, 2025b).
Patients with aspirin-exacerbated asthma typically present with nasal congestion and anosmia (loss of smell), leading to chronic rhinosinusitis with nasal polyps and, eventually, asthma. They usually describe acute exacerbations within 60–120 minutes of exposure to aspirin or other NSAIDs, along with rhinorrhea, nasal obstruction, conjunctival irritation, and flushing of the head and neck. If needed, it can be confirmed with an aspirin challenge test in a well-monitored environment with access to emergency equipment. NSAIDs should be avoided in these patients, but COX-2 inhibitors or acetaminophen (Tylenol) are typically well tolerated. Asthma symptoms can be treated with ICS, LTRA, with or without oral corticosteroids, and desensitization therapy (GINA, 2025b).
Referral to a Specialist
Recognizing when a patient needs referral to a specialist for more advanced care should be of utmost concern to the provider. In patients aged 4 and under, the EPR-4 suggests referral to an asthma specialist if step 3 management or higher is reached, with consideration at step 2. In patients aged 5 and above, this threshold is step 4 or higher, with consideration in step 3 (NHLBI, 2020a). GINA guidelines recommend referral to an asthma specialist at step 5 or in the following circumstances:
- difficulty confirming or doubts regarding the diagnosis
- suspected occupational asthma
- persistent severely uncontrolled asthma or frequent exacerbations despite correct inhaler technique and adherence to treatment
- the presence of any risk factors for asthma-related death, such as ICU admission, mechanical ventilation, anaphylaxis, or a confirmed food allergy
- the risk for or evidence of significant treatment adverse effects (in children, growth delay)
- symptoms that are suggestive of complications or subtypes of asthma, such as aspirin-exacerbated respiratory disease or allergic bronchopulmonary aspergillosis (GINA, 2025a, 2025b).
References
Ali, H., Rasya, S. F. W., & Siregar, M. A. G. (2023). The potential of fractional exhaled nitric oxide as a biomarker in predicting and optimizing use of treatment in asthma. South East European Journal of Immunology, 6(1), 18–23. https://doi.org/10.3889/seejim.2023.6033
Allergy & Asthma Network. (n.d.-a). Understanding eosinophilic asthma: Symptoms, diagnosis, and treatment options. Retrieved March 16, 2026, from https://allergyasthmanetwork.org/what-is-asthma/eos-asthma/
Allergy & Asthma Network. (n.d.-b). What is asthma? Retrieved March 16, 2026, from https://allergyasthmanetwork.org/what-is-asthma/
Allergy & Asthma Network. (2025a). School-based allergies and asthma management program becomes law! https://allergyasthmanetwork.org/news/action-alert-u-s-house-of-representatives-passes-h-r-2468-the-school-based-allergies-and-asthma-management-program-act/
Allergy & Asthma Network. (2025b). USAsthma summit 2025: What does the future of asthma care look like? Retrieved March 16, 2026, from https://allergyasthmanetwork.org/news/usasthma-summit-2025/
American Academy of Allergy Asthma & Immunology. (2024). SMART therapy for asthma. https://www.aaaai.org/tools-for-the-public/conditions-library/asthma/smart
American Academy of Allergy Asthma & Immunology. (2025). The school-based allergy, asthma and anaphylaxis management program®: Comprehensive asthma educational resources. Retrieved March 16, 2026, from https://www.aaaai.org/tools-for-the-public/school-tools/sampro
American Lung Association. (2024). Spirometry implementation quick glance guide. https://www.lung.org/getmedia/d53c0e59-f3ab-435a-bcaa-a6a195b6b565/spirometry-quick-glance-guide.pdf
American Lung Association. (2026a). Breathing exercises. https://www.lung.org/lung-health-and-diseases/protecting-your-lungs/breathing-exercises.html
American Lung Association. (2026b). Create an asthma action plan. https://www.lung.org/lung-health-diseases/lung-disease-lookup/asthma/managing-asthma/create-an-asthma-action-plan
Asthma and Allergy Foundation of America. (2024). Allergens and allergic asthma. https://www.aafa.org/allergic-asthma
Asthma and Allergy Foundation of America. (2025a). 2025 asthma capitals: The most challenging places to live with asthma. https://aafa.org/wp-content/uploads/2025/09/aafa-2025-asthma-capitals-report.pdf
Asthma and Allergy Foundation of America. (2025b). With asthma-related ER visits increasing, AAFA names 2025 asthma capitals. https://aafa.org/with-asthma-related-er-visits-increasing-aafa-names-2025-asthma-capitals/
Baan, E. J., Hoeve, C. E., De Ridder, M., Demoen, L., Lahousse, L., Brusselle, G. G., & Verhamme, K. M. C. (2021). The ALPACA study: (In)appropriate LAMA prescribing in asthma: A cohort analysis. Pulmonary Pharmacology & Therapeutics, 71, 102074. https://doi.org/10.1016/j.pupt.2021.102074
Barry, T., Holliday, M., Sparks, J., Biggs, R., Colman, A., Lamb, R., Oldfield, K., Shortt, N., Kerse, K., Martindale, J., Eathorne, A., Walton, M., Black, B., Harwood, M., Bruce, P., Semprini, R., Bush, A., Fleming, L., Byrnes, C. A., … Beasley, R. (2024). START CARE: a protocol for a randomised controlled trial of step-wise budesonide-formoterol reliever-based treatment in children. ERJ Open Research, 10(2), 00897-2023. https://doi.org/10.1183/23120541.00897-2023
Beasley, R., Bruce, P., Houghton, C., & Hatter, L. (2023). The ICS/formoterol reliever therapy regimen in asthma: A review. The Journal of Allergy and Clinical Immunology: In Practice, 11(3), 762–772. https://doi.org/10.1016/j.jaip.2023.01.002
Cardet, J. C., Papi, A., & Reddel, H. K. (2023). “As-Needed” inhaled corticosteroids for patients with asthma. The Journal of Allergy and Clinical Immunology In Practice, 11(3), 726–734. https://doi.org/10.1016/j.jaip.2023.01.010
Casale, T. B., Foggs, M. B., & Balkissoon, R. C. (2022). Optimizing asthma management: Role of long-acting muscarinic antagonists. Journal of Allergy and Clinical Immunology, 150(3), 557–568. https://doi.org/10.1016/j.jaci.2022.06.015
Centers for Disease Control and Prevention. (2022a). Uncontrolled asthma among adults, 2019. https://archive.cdc.gov/#/details?url=https://www.cdc.gov/asthma/asthma_stats/uncontrolled-asthma-adults-2019.htm
Centers for Disease Control and Prevention. (2022b). Uncontrolled asthma among children with current asthma, 2018-2020. https://archive.cdc.gov/#/details?url=https://www.cdc.gov/asthma/asthma_stats/uncontrolled-asthma-children-2018-2020.htm
Centers for Disease Control and Prevention. (2023). Most recent national asthma data. https://www.cdc.gov/asthma/most_recent_national_asthma_data.htm
Centers for Disease Control and Prevention. (2024). Control asthma. https://archive.cdc.gov/#/details?url=https://www.cdc.gov/sixeighteen/asthma/index.htm
Centers for Disease Control and Prevention. (2026). Asthma. https://www.cdc.gov/nchs/fastats/asthma.htm
Chambers, C. D., Krishnan, J. A., Alba, L., Albano, J. D., Bryant, A. S., Carver, M., Cohen, L. S., Gorodetsky, E., Hernandez-Diaz, S., Honein, M. A., Jones, B. L., Murray, R. K., Namazy, J. A., Sahin, L., Spong, C. Y., Vasisht, K. P., Watt, K., Wurst, K. E., Yao, L., & Schatz, M. (2021). The safety of asthma medications during pregnancy and lactation: Clinical management and research priorities. Journal of Allergy and Clinical Immunology, 147(6), 2009-2020. https://doi.org/10.1016/j.jaci.2021.02.037
Chupp, G., Kline, J. N., Khatri, S. B., McEvoy, C., Silvestri, G. A., Shifren, A., Castro, M., Bansal, S., McClelland, M., Dransfield, M., Trevor, J., Kahlstrom, N., Simoff, M., Wahidi, M. M., Lamb, C. R., Ferguson, J. S., Haas, A., Hogarth, D. K., Tejedor, R., … Laviolette, M. (2021). Bronchial thermoplasty in patients with severe asthma at 5 years. Chest Journal, 161(3), 614–628. https://doi.org/10.1016/j.chest.2021.10.044
Czira, A., Turner, M., Martin, A., Hinds, D., Birch, H., Gardiner, F., & Zhang, S. (2022). A systematic literature review of burden of illness in adults with uncontrolled moderate/severe asthma. Respiratory Medicine, 191, 106670. https://doi.org/10.1016/j.rmed.2021.106670
Di Cicco, M. E., Peroni, D., Marseglia, G. L., & Licari, A. (2025). Unveiling the complexities of pediatric asthma treatment: Evidence, controversies, and emerging approaches. Pediatric Drugs, 27, 393–404. https://doi.org/10.1007/s40272-025-00694-6
Garn, H., Potaczek, D. P., & Pfefferle, P. I. (2021). The hygiene hypothesis and new perspectives—Current challenges meeting an old postulate. Frontiers in Immunology, 12, 637087. https://doi.org/10.3389/fimmu.2021.637087
Global Initiative for Asthma. (2025a). 2025 GINA difficult-to-treat & severe asthma guide. https://ginasthma.org/wp-content/uploads/2025/11/GINA-Severe-Asthma-Guide-2025-WEB-FINAL-WMS.pdf
Global Initiative for Asthma. (2025b). Global strategy for asthma management and prevention. https://ginasthma.org/wp-content/uploads/2025/11/GINA-2025-Update-25_11_08-WMS.pdf
Gruenwald, T., Seals, B. A., Knibbs, L. D., & Hosgood III, H. D. (2023). Population attributable fraction of gas stoves and childhood asthma in the United States. International Journal of Environment Research and Public Health, 20(1), 75. https://doi.org/10.3390/ijerph20010075
Hartert, T., & Bacharier, L. B. (2025). An overview of asthma management in children and adults. UpToDate. Retrieved March 16, 2026, from https://www.uptodate.com/contents/an-overview-of-asthma-management-in-children-and-adults
Heaney, L. G., de Llano, L. P., Al-Ahmad, M., Backer, V., Busby, J., Canonica, G. W., Christoff, G. C., Cosio, B. G., FitzGerald, J. M., Heffler, E., Iwanaga, T., Jackson, D. J., Menzies-Gow, A. N., Papadopoulos, N. G., Papaioannou, A. I., Pfeffer, P. E., Popov, T. A., Porsbjerg, C., Rhee, C. K., … Price, D. B. (2021). Eosinophilic and noneosinophilic asthma, an expert consensus framework to characterize phenotypes in a global real-life asthma cohort. Chest Journal, 160(3), 814-830. https://doi.org/10.1016/j.chest.2021.04.013
Hussain, M., & Liu, G. (2024). Eosinophilic asthma: Pathophysiology and therapeutic horizons. Cells, 13(5), 384. https://doi.org/10.3390/cells13050384
Irvin, C. G. (2026). Pulmonary function testing in asthma. UpToDate. Retrieved March 16, 2026, from https://www.uptodate.com/contents/pulmonary-function-testing-in-asthma
Kalayci, O., Miligkos, M., Beltrán, C. F. P., El-Sayed, Z. A., Gómez, R. M., Hossny, E. Le Souef, P. Nieto, A., Phipatanakul, W., Pitrez, P. M., Xepapadaki, P., Jiu-Yao, W., & Papadopoulos, N. G. (2022). The role of environmental allergen control in the management of asthma. World Allergy Organization Journal, 15(3), 100634. https://doi.org/10.1016/j.waojou.2022.100634
Khan, S., Herndon, T. M., Keswani, A., Clarridge, K., Pisal, D. S., Ji, P., Kim, J., Klein, M., Chin, S., Sahajwalla, C., & Stone, K. D. (2026). Food and Drug Administration regulation of biosimilar products: Improving affordability of biologics for patients with asthma and allergic diseases. Journal of Allergy and Clinical Immunology. S0091-6749(26)00182-X. Advance online publication. https://doi.org/10.1016/j.jaci.2026.02.041
Lamb, K., Theodore, D., & Bhutta, B. S. (2023). Spirometry. In StatPearls [Internet]. StatPearls Publishing. Retrieved March 16, 2026, from https://www.ncbi.nlm.nih.gov/books/NBK560526
Leung, C., & Sin, D. D. (2026). Add-on LAMA therapy in asthma: An underused strategy for exacerbation prevention. The Lancet, Respiratory Medicine, 14(4), 288–289. https://doi.org/10.1016/S2213-2600(26)00006-8
Liang, T. Z., & Chao, J. H. (2023). Inhaled corticosteroids. In StatPearls [Internet]. StatPearls Publishing. Retrieved March 16, 2026, from https://www.ncbi.nlm.nih.gov/books/NBK470556
Litonjua, A. A., & Weiss, S. T. (2025). Epidemiology of asthma. UpToDate. Retrieved March 18, 2026, from https://www.uptodate.com/contents/epidemiology-of-asthma
Liu, M., Wang, J., & Sun, X. (2022). A meta-analysis on vitamin D supplementation and asthma treatment. Frontiers in Nutrition, 9, 860628. https://doi.org/10.3389/fnut.2022.860628
Maciag, M. C., & Phipatanakul, W. (2022). Update on indoor allergens and their impact on pediatric asthma. Annals of Allergy, Asthma & Immunology, 128(6), 652–658. https://doi.org/10.1016/j.anai.2022.02.009
Mahay, G., Zysman, M., Guibert, N., Barnig, C., Guilleminault, L., & Dupin. (2025). Long-acting muscarinic antagonists (LAMA) in asthma: What is the best strategy? Respiratory Medicine and Research, 87, 101157. https://doi.org/10.1016/j.resmer.2025.101157
Mammen, J. R. (2021). Focused summary (2021) of updated guidelines for asthma management of adults and children ages 12+. https://digitalcommons.uri.edu/cgi/viewcontent.cgi?article=1000&context=oer-healthcare-asthma
Marcon, A., Martinelli, L., Bansal, A. T., Berret, E., Bossios, A., Marchetti, P., Porsbjerg, C., Principe, S., Schleich, F., Sergejeva, S., Sont, J. K., & Caminati, M. (2025). Use of long-acting muscarinic antagonists for severe asthma: Insights from clinicians in the SHARP network. Respiratory Research, 26, 306. https://doi.org/10.1186/s12931-025-03378-4
Mazi, A., Madani, F., Alsulami, E., Almutari, A., Alamri, R., Jahhaf, J., & Alsulaimani, S. (2023). Uncontrolled asthma among children and its association with parents’ asthma knowledge and other socioeconomic and environmental factors. Cureus, 15(2), e35240. https://doi.org/10.7759/cureus.35240
Minutello, K., & Gupta, V. (2024). Cromolyn sodium. In StatPearls [Internet]. StatPearls Publishing. Retrieved March 16, 2026, from https://www.ncbi.nlm.nih.gov/books/NBK557473
National Heart, Lung, and Blood Institute. (2007). National asthma education and prevention program: Expert panel report 3: Guidelines for the diagnosis and management of asthma. https://www.nhlbi.nih.gov/sites/default/files/media/docs/EPR-3_Asthma_Full_Report_2007.pdf
National Heart, Lung, and Blood Institute. (2013a). Peak expiratory flow meter [image]. Wikimedia. https://commons.wikimedia.org/wiki/File:Peak_expiratory_flow_meter-pediatric_use.PNG
National Heart, Lung, and Blood Institute. (2013b). Spirometry testing [image]. Wikimedia. https://commons.wikimedia.org/wiki/File:Spirometry_NIH.jpg
National Heart, Lung, and Blood Institute. (2020a). 2020 focused updates to the asthma management guidelines: A report from the national asthma education and prevention program coordinating committee expert panel working group. https://www.nhlbi.nih.gov/resources/2020-focused-updates-asthma-management-guidelines
National Heart, Lung, and Blood Institute. (2020b). 2020 focused updates to the asthma management guidelines: At-a-glance guide [Image] (NIH Publication No. 12-5075). https://www.nhlbi.nih.gov/resources/at-glance-2020-focused-updates-asthma-management-guidelines
National Heart, Lung, and Blood Institute. (2021). Asthma action plan (NIH Publication No. 20-HL-5251). https://www.nhlbi.nih.gov/sites/default/files/publications/Asthma-Action-Plan-2020_rev_508.pdf
National Heart, Lung, and Blood Institute. (2024). Asthma: What is asthma? https://www.nhlbi.nih.gov/health/asthma
Ortega, V. E., & Chiarella, S. E. (2026a). Asthma. Merck Manual Professional Version. https://www.merckmanuals.com/professional/pulmonary-disorders/asthma-and-related-disorders/asthma
Ortega, V. E., & Chiarella, S. E. (2026b). Pharmacologic treatment of asthma. Merck Manual Professional Version. https://www.merckmanuals.com/professional/pulmonary-disorders/asthma-and-related-disorders/pharmacologic-treatment-of-asthma
Pate, C. A., & Zahran, H. S. (2024). The status of asthma in the United States. Preventing Chronic Disease, 21, 240005. https://doi.org/10.5888/pcd21.240005
Perrem, L., Gaietto, K., Weiner, D. J., & Rosenfeld, M. (2024). Advances in pediatric lung function testing techniques. Clinics in Chest Medicine, 45(3), 543–553. https://doi.org/10.1016/j.ccm.2024.03.003
Popovic-Grle, S., Stajduhar, A., Lampalo, M., & Rnjak, D. (2021). Biomarkers in different asthma phenotypes. Genes, 12(6), 801. https://doi.org/10.3390/genes12060801
Porpodis, K., Tsiouprou, I., Apostolopoulos, A., Ntontsi, P., Fouka, E., Papakosta, D., Vliagoftis, H., & Domvri, K. (2022). Eosinophilic asthma, phenotypes-endotypes and current biomarkers of choice. Journal of Personalized Medicine, 12(7), 1093. https://doi.org/10.3390/jpm12071093
Rogers, J. L., & Brashers, V. L. (Eds.). (2023). McCance and Huether’s pathophysiology: The biologic basis for disease in adults and children (9th ed.). Elsevier.
Rosen, D. M., & Colin, A. A. (2025). Overview of pulmonary function testing in children. UpToDate. Retrieved March 17, 2026, from https://www.uptodate.com/contents/overview-of-pulmonary-function-testing-in-children
Sayeedi, I., Goldin, J., & Widrich, J. (2025). Methacholine challenge test. In StatPearls [Internet]. StatPearls Publishing. Retrieved March 17, 2026, from https://www.ncbi.nlm.nih.gov/books/NBK547716
Schatz, M., & Weinberger, S. E. (2023). Management of asthma during pregnancy. UpToDate. Retrieved March 16, 2026, from https://www.uptodate.com/contents/management-of-asthma-during-pregnancy
Sharma, S., & Carr, T. F. (2026). Treatment of severe asthma in adolescents and adults. UpToDate. Retrieved March 16, 2026, from https://www.uptodate.com/contents/treatment-of-severe-asthma-in-adolescents-and-adults
Sharma, S., & Chakraborty, R. K. (2023). Asthma medications. In StatPearls [Internet]. StatPearls Publishing. Retrieved March 17, 2026, from https://www.ncbi.nlm.nih.gov/books/NBK531455
Shebl, E., & Chakraborty, R. K. (2023). Asthma in pregnancy. In StatPearls [Internet]. StatPearls Publishing. Retrieved March 16, 2026, from https://www.ncbi.nlm.nih.gov/books/NBK532283
Sinyor, B., & Perez, L. C. (2023). Pathophysiology of asthma. In StatPearls [Internet]. StatPearls Publishing. Retrieved March 17, 2026, from https://www.ncbi.nlm.nih.gov/books/NBK551579
Slob, E. M. A., Vijverberg, S. J. H., Ruffles, T., Noij, L. C. E., Biermann, J., Brouwer, A. F. J., van den Brink, K., de Bruin-Kok, A., Van Ewijk, B. E., Haarman, E., Hammer, S. C., Hashimoto, S., Hogarth, F., Jones, C. J., Kamps, A. W. A., Kersten, E. T. G., de Kleer, I., Lipworth, B. J., Littleford, R., … Maitland-van der Zee, A. H. (2025). Genotype-guided asthma treatment reduces exacerbations in children: Meta-analysis of two randomized control trials. Allergy, 80(4), 1006–1014. https://doi.org/10.1111/all.16438
Sobieraj, D. M., Baker, W. L., Nguyen, E., Weeda, E. R., Coleman, C. I., White, C. M., Lazarus, S. C., Blake, K. V., & Lang, J. E. (2018a). Association of inhaled corticosteroids and long-acting muscarinic antagonists with asthma control in patients with uncontrolled, persistent asthma: A systematic review and meta-analysis. JAMA, 319(14), 1473–1484. https://doi.org/10.1001/jama.2018.2757
Sobieraj, D. M., Baker, W. L., Weeda, E. R., Nguyen, E., Coleman, C. I., White, C. M., Lazarus, S. C., Blake, K. V., & Lang, J. E. (2018b). Intermittent inhaled corticosteroids and long-acting muscarinic antagonists for asthma. Agency for Healthcare Research and Quality. https://pubmed.ncbi.nlm.nih.gov/29741837/
UpToDate Lexidrug. (n.d.). Tezepelumab: Drug information. UpToDate. Retrieved March 16, 2026, from https://www.uptodate.com/contents/tezepelumab-drug-information
US Department of Health and Human Services. (2020). 2020 focused updates to the asthma management guidelines. https://www.nhlbi.nih.gov/health-topics/asthma-management-guidelines-2020-updates
US Food and Drug Administration. (2012). MDI with attached spacer device [Image]. https://www.flickr.com/photos/fdaphotos/7349095984/in/photostream
Wang, Z., Pianosi, P., Keogh, K., Zaiem, F., Alsawas, M., Alahdab, F., Almasri, J. M., Mohammed, K., Larrea-Mantilla, L., Farah, W., Daraz, L., Barrionuevo, P., Gunjal, S., Prokop, L. J., & Murad, M. H. (2017). The clinical utility of fractional exhaled nitric oxide (FeNO) in asthma management. Agency for Healthcare Research and Quality. https://www.ncbi.nlm.nih.gov/sites/books/NBK487485/
Wood, K. L. (2024). Airflow, lung volumes, and flow-volume loop. Merck Manual Professional Version. https://www.merckmanuals.com/professional/pulmonary-disorders/tests-of-pulmonary-function-pft/airflow-lung-volumes-and-flow-volume-loop
Woods, A. D. (2023). Nursing2023 drug handbook (43rd ed.). Wolters Kluwer.
World Health Organization. (2024). Asthma. https://www.who.int/news-room/fact-sheets/detail/asthma
Powered by Froala Editor