About this course:
This activity aims to examine bereavement in nurses following the death of a patient, highlighting the manifestations of grief and consequences of unresolved grief, as well as strategies to help nurses cope with grief in a healthy manner to prevent compassion fatigue and promote physical and mental health and well-being.
Course preview
Coping With Patient Death as a Nurse
This activity aims to examine bereavement in nurses following the death of a patient, highlighting the manifestations of grief and consequences of unresolved grief, as well as strategies to help nurses cope with grief in a healthy manner to prevent compassion fatigue and promote physical and mental health and well-being.
Upon completion of this module, learners should be able to:
- define terminology related to end-of-life care, death, and dying
- review theories of grief, the five stages of grief, and compare the different types of grief
- describe the signs and symptoms of grief and discuss the distinction between prolonged grief disorder and normal grieving
- explain how grief can manifest in nurses and identify the consequences of unhealthy grieving, including compassion fatigue and burnout
- identify personal and organizational strategies for helping nurses cope with grief and death, and the impact of emotional resiliency on grieving
Nurses assume various roles throughout a patient’s illness trajectory, whether it be an unexpected, acute illness necessitating care in the intensive care unit (ICU) or an extended period of chronic disease such as cancer. Regardless of the setting or precipitating event, nurses are routinely faced with death and dying in clinical practice and tasked with caring for patients and families at the end of life (EOL). Nurses continue to provide comprehensive and compassionate care at the EOL, with responsibilities grounded in evidence-based nursing practice and clinical ethics. Nurses foster a therapeutic environment by managing the physical and psychosocial aspects of dying; alleviating pain and suffering; enhancing the quality of life; addressing the patient’s psychological, emotional, and spiritual needs; and preserving dignity. Nursing care at the EOL eases the transition from curative, life-saving interventions to palliative or hospice-focused care. Since the goal of EOL or hospice care is no longer to cure disease and restore health, nurses shift their energy to focus on satisfying complex needs throughout the dying process. Nursing care provided during this poignant period often facilitates intimate nurse–patient–family relationships. Strong emotional bonds and attachment can develop for the patient, family, and nurse, fostering a positive death experience for the patient and their loved ones. While nurses can derive a sense of satisfaction and fulfillment from these connections, the death of a patient can also have a profound and painful impact. Some nurses may experience overwhelming emotions, such as heartache, despair, and grief. Without the proper skill set, training, or support system, the nurse’s emotional, psychological, and physical health and welfare may become compromised. Nurses must maintain emotional resiliency to continue providing patients with high-quality and compassionate care (American Nurses Association [ANA], 2024a; Potter et al., 2026, pp. 136–137; Yarbro et al., 2018).
Defining Terminology
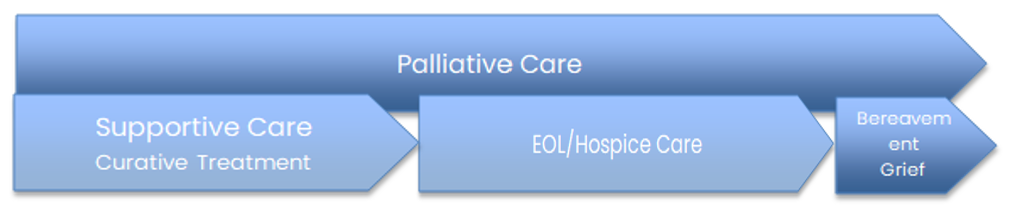
The World Health Organization (WHO, 2023) defines palliative care as an approach that improves the quality of life of patients (adults and children) and their families who are facing problems associated with a life-threatening illness. It prevents and relieves suffering through the early identification, correct assessment, and treatment of pain and other problems, whether physical, psychosocial, or spiritual (para. 1). Palliative care should expand across the continuum of illness and is based on the patient’s needs, not the patient’s prognosis. Palliative care can be implemented at any stage of illness and delivered alongside supportive or curative treatment. Palliative care does not hasten death and is not intended to prolong the dying process; rather, it focuses on improving quality of life by reducing symptom burden and suffering so that patients may live as well as possible for as long as possible with serious illness (Center to Advance Palliative Care [CAPC], n.d.). The term supportive care is sometimes used interchangeably with palliative care; however, it more commonly describes interventions aimed at preventing and managing symptoms and treatment-related side effects, particularly for patients undergoing active therapy. In oncology, for example, supportive care may include blood product support or antiemetic therapy during chemotherapy. In infectious disease, supportive care may refer to adequate rest, hydration, and nutrition required for a patient whose immune system is actively fighting a viral infection. Supportive care can overlap with palliative care and may evolve as goals of care shift over time. The National Cancer Institute (NCI, n.d.) defines EOL care as the care provided to individuals with a terminal illness who are approaching death, either because they have chosen to forgo life-prolonging, curative treatment or because no further disease-directed treatment options are available. The term embodies the delivery of care within four domains: physical comfort, social needs, emotional support, and spiritual issues. The primary goal of EOL care is to promote comfort by managing symptoms, such as pain or dyspnea, throughout the dying process, which is why EOL care is also referred to as comfort care. Hospice care is the most intensive, refined form of EOL care implemented, reserved for terminally ill patients with a life expectancy of 6 months or less. Electing hospice acknowledges that attempts to cure or slow disease progression have failed or resulted in greater burden than benefit, and that time is limited. Death is the expected outcome of hospice, and the preeminent goals include enhancing the quality of life, aiding in comfort, alleviating suffering, and providing emotional and spiritual support for patients and their families (Meier, 2025; Potter et al., 2026, p. 798; Yarbro et al., 2018). For additional detailed information on these topics, please refer to the NursingCE courses entitled Ethical Considerations at the End of Life and Palliative Care.
Bereavement refers to the objective state of having experienced a significant loss, most commonly through the death of a loved one. The word’s root form means to be shorn off, indicating that something has been removed or stripped away. Bereavement can be profoundly disruptive, yet it remains a universal and normal human experience. Grief is the reaction to a loss, either actual or perceived. It is a person’s thoughts and feelings, as well as their physical, behavioral, or spiritual response to the loss of something or someone that was valued. Grief is highly variable and is not experienced or expressed in the same way by different individuals; however, all people will experience grief and loss at some point in their lives. The term mourning is closely related to grief and is sometimes misused as a synonym for grief. Whereas grief is the reaction to a loss, mourning is the process where a grieving person incorporates the loss into their everyday life or the external or public expression of grief. Prime examples of...
...purchase below to continue the course
Figure 1
Concepts related to the care of patients across the illness trajectory
Theories of Grief
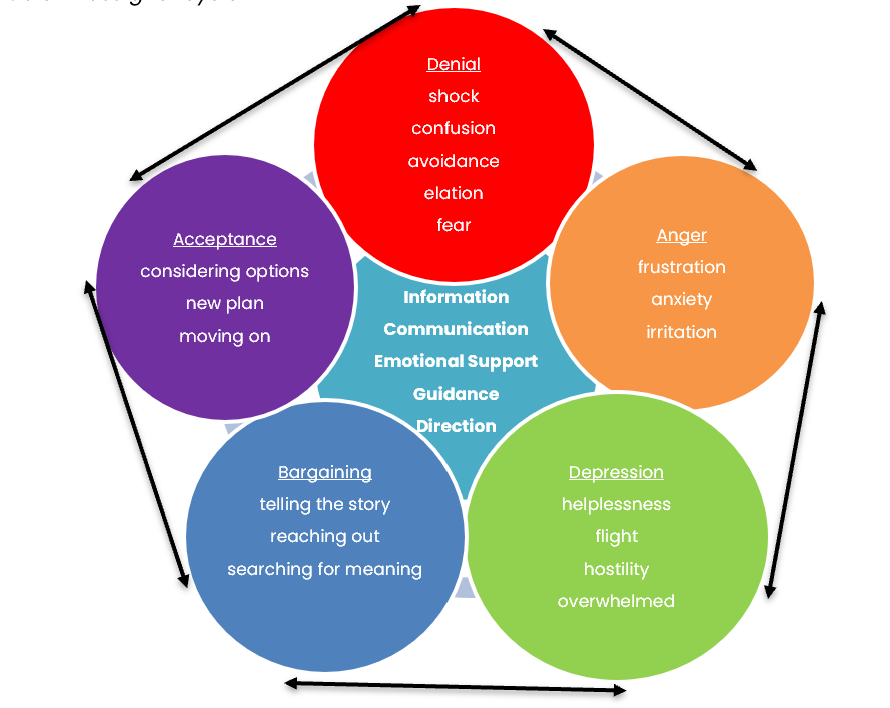
Sigmund Freud proposed one of the earliest grief theories in his 1917 publication, Mourning and Melancholia. Freud’s theory is premised on the concept of working through grief. His work centered on letting go of the bonds and attachment to those who have died, acclimating to a new sphere of normalcy without the deceased, and building new relationships and experiences (DeSpelder et al., 2020; Freud, 1917). In 1969, Elisabeth Kübler-Ross proposed the stage theory by publishing her book, On Death and Dying. This book represented the culmination of hundreds of interviews with dying patients through which she cultivated the theory that there are five stages to death and dying: denial, anger, bargaining, depression, and acceptance (frequently referred to as DABDA). Originally developed to explain the stages patients go through after receiving a terminal or life-limited diagnosis, it was later applied to postdeath or postloss experiences. The Kübler-Ross model has profoundly impacted the world and is among the most well-known and commonly taught systems for understanding the grieving process. Despite Kübler-Ross stating in her book that the stages can occur in any order and some simultaneously (i.e., overlap, concurrently), it received criticism for being a linear model by those who did not understand or read the text thoroughly. The concepts have since been clarified to make clear that the emotional states and adaptive mechanisms associated with the five stages of grief occur in a variety of patterns. Some people will not go through each stage, whereas others may repeat stages. The stages often overlap, as they are not consecutive, isolated experiences for most people (Potter et al., 2026, p. 788; Tyrrell et al., 2023). Figure 2 provides further insight into each stage’s underlying emotions and concepts.
Figure 2
Kübler-Ross grief cycle
Signs of Grief
The signs and symptoms of grief vary widely interpersonally and intrapersonally. In addition to those highlighted in Figure 2, grief can manifest across a spectrum of emotions, feelings, physical sensations, and behaviors. People who are grieving experience sadness and sorrow commonly, which may or may not be expressed by crying. Feelings of disbelief, helplessness, numbness, and shock are common. These feelings primarily serve as defense mechanisms to safeguard the bereaved from feeling overwhelmed by the pain of the loss. Guilt is common and may be related to survivor’s guilt, unfinished business, or grounded in irrational thoughts that the death could have somehow been prevented. Some people may feel emotionally isolated and detached from others, whereas others may intentionally distance themselves from others to protect against being hurt by the loss of another person. Grief’s most common physical manifestations include fatigue, exhaustion, insomnia, headaches, joint pain, dry mouth, muscle aches, and gastrointestinal ulcers. Anxiety is one of the most common emotions experienced following the death of a loved one. It is often accompanied by nausea, anorexia, chest tightness, irritability, and restlessness. Cognitive manifestations can include excessive worry, fear, feelings of impending doom, an inability to concentrate, and a sense of confusion. People may become preoccupied with the deceased, and some describe hallucinations. Behavioral symptoms can involve withdrawal in the form of emotional or physical detachment from others. Performance at work or school may become impaired, and the bereaved may avoid any setting, situation, or circumstance that reminds them of the deceased (NCI, 2024; Schoo et al., 2025; Shear et al., 2026).
Types of Grief
There are several types of grief responses; some are considered normal and indicative of healthy grieving, whereas others suggest maladaptive coping with loss. The most common types of grief are described in this section.
Normal (Uncomplicated) Grief
Normal grief is considered the typical and universal reaction to loss. Approximately 2.5 million people in the United States die each year, leaving behind around five to nine close relatives and friends to grieve (Potter et al., 2026, p. 787; Shear et al., 2026). Normal or uncomplicated grief often includes a variety of signs and symptoms from the physical, emotional, cognitive, or behavioral domains of loss. Normal grieving centers on the decrease of grief-related symptoms and the gradual movement toward acceptance of the loss, as the bereaved eventually adjust to the loss and move forward with life. There is no defined or universal timeframe for grieving, as the process is highly individualized and influenced by factors such as the nature of the loss, the relationship with the deceased, cultural context, and available support. However, many individuals demonstrate significant adjustment within the first 6–12 months following a loss. Although grief may persist beyond this period, a typical grief trajectory reflects gradual movement toward integration, growth, and healing rather than complete resolution of grief (NCI, 2024; Potter et al., 2026, p. 787; Shear et al., 2026).
In 2022, the most recent version of the Diagnostic and Statistical Manual of Mental Disorders Text Revision (DSM-5-TR) added prolonged grief disorder as a diagnosis for individuals who experience persistent and impairing grief responses. Previously, this was termed persistent complex bereavement disorder. It is estimated that 4%–15% of adults will meet the criteria of prolonged grief disorder following a loss. Critics have raised concerns that the diagnostic criteria may insufficiently account for individual, cultural, and contextual differences in normative grief responses and grieving duration (American Psychiatric Association [APA], 2022, 2025; Prigerson et al., 2024). Table 1 outlines the specific aspects of normal grieving in direct comparison to the clinical features of prolonged grief disorder as defined by the APA in the DSM-5-TR.
Table 1
DSM-5-TR Comparison of Normal Grieving and Prolonged Grief Disorder
Normal Grieving | Prolonged Grief Disorder |
Painful feelings come in waves, lessen in intensity and frequency over time, and are intermingled with positive memories of the deceased person. | Symptoms persist for 12 months or more after the death for adults and 6 months or more for children and adolescents, with little improvement. |
Predominant experiences include emptiness and loss, accompanied by occasional pleasant emotions. | Intense longing or yearning for the deceased or daily preoccupation with the deceased. |
Self-esteem is usually preserved. | Feeling like part of oneself has died (identity disruption). |
Thoughts of death and dying are usually focused on the deceased, reuniting with the deceased in death, or feelings of guilt toward specific gaps or failures in the relationship with the deceased. | Persistent emotional numbness, difficulty accepting the death, and persistent disbelief. |
The individual maintains connections with family and friends, particularly those who can console the bereaved person. | Avoidance of anything that is a reminder of loss, difficulty functioning in life, or marked emotional pain, such as bitterness and anger. |
Can imagine the future and hope is retained. | Extreme loneliness, loss of meaning in life, or a feeling of detachment from others. |
Mild functional impairment improves with time. | Clinically significant impairment in occupation, social, or other critical areas of functioning. |
(APA, 2022; Potter et al., 2026, p. 787; Shear et al., 2026)
Anticipatory Grief
Anticipatory grief is a response to an expected death and can start at the time of diagnosis and continue until the person dies. Anticipatory grief includes many of the same symptoms of normal grieving following death, but the distinction is that the ill person is still alive and present when the grieving begins. Anticipatory grief can be experienced by a loved one or the person expected to die. It is commonly experienced by family members of loved ones diagnosed with a chronic or terminal illness who grieve while the patient is alive due to an awareness of the impending loss. Individuals who are dying can also experience anticipatory grief, foreseeing the loss of function, independence, or future absence from major life events, such as their children’s marriage or their grandchildren’s birth. This can be highly distressing to patients and accompanied by anxiety, fear, and heightened perceived pain levels (DeSpelder et al., 2020; Potter et al., 2026, p. 787; Shear et al., 2026). Not all patients with a terminal illness will experience anticipatory grief. According to the NCI (2024), approximately 25% of patients with incurable cancer experienced anticipatory grief. Certain factors, such as dependent relationships, limited social support, and spiritual or existential distress, have been associated with a greater likelihood of anticipatory grief, while acceptance of impending death by the patient and their social network may mitigate its intensity. Research suggests that anticipatory grief may serve a meaningful role for some patients and families by facilitating emotional preparation and acceptance. However, its impact on postdeath bereavement varies, and anticipatory grief does not universally reduce the experience of distress after death. Adaptive outcomes depend on individual coping styles, the quality of support, and the degree to which grief is acknowledged and processed (NCI, 2024).
Complicated Grief
Complicated grief is precisely as it sounds: more complex and challenging to navigate and potentially requiring professional help to manage depending on its severity. The feelings of loss are debilitating and show little improvement over time compared with normal grief. Instead, the bereaved person has significant difficulty recovering from the loss and resuming their life. Complicated grief is often characterized by anger and bitterness, recurrent painful emotions, and difficulty accepting the reality of the death. The bereaved are often preoccupied with thoughts of the deceased, unable to focus on anything other than the loss, experience distressing or intrusive thoughts related to the death, and have an intense yearning and longing for the deceased. The bereaved may lose the meaning associated with their life and a sense of purpose, making it difficult to carry out normal daily activities (Potter et al., 2026, pp. 787–788). The term complicated grief is commonly used in nursing to describe patterns of maladaptive or prolonged grieving that interfere with functioning. While these patterns are not included as a medical diagnosis in the DSM-5-TR, they remain clinically useful for nursing assessment, early identification of risk, and guiding supportive interventions. In contrast, prolonged grief disorder is a formal medical diagnosis in the DSM-5-TR with specific symptoms and timing criteria. Table 2 outlines four commonly recognized patterns of complicated grief.
Table 2
Four Patterns of Complicated Grief
Pattern | Description |
Chronic | Normal grief that continues for an extended or prolonged period without sufficient resolution. |
Delayed | Normal grief reactions are suppressed or postponed (consciously or unconsciously) to avoid the pain, with symptoms emerging much later than expected. |
Exaggerated | An intense reaction to loss that can include suicidal ideation, phobias, or night terrors; a pattern characterized by extreme or atypical symptoms. |
Masked | The affected individual is unaware that their behaviors are related to the loss and shows limited recognizable separation distress or typical grief features. |
(NCI, 2024; Potter et al., 2026, p. 788)
Certain situations and factors can increase the risk of an individual experiencing complicated grief (DeSpelder et al., 2020). Examples include:
- enduring repeated loss or deaths that are sudden, traumatic, violent, or random, such as fatal accidents, homicide, or suicidal ideation
- a death that is drawn out due to a long-term illness
- the death of a child
- believing that the death was preventable
- presence of a psychiatric condition
- a relationship between the deceased and bereaved that is dependent or ambivalent (DeSpelder et al., 2020)
Additional risk factors for complicated grief include a lack of social support, survivors of age younger than 60, lower income, a history of depression, and concurrent life stressors (DeSpelder et al., 2020; NCI, 2024).
Disenfranchised Grief
Disenfranchised grief occurs when a loss is not openly acknowledged, socially validated, or supported, leaving the grieving individual feeling isolated or invalidated in their response. It may arise when the relationship to the deceased is unrecognized, the loss itself is minimized, the griever is perceived as incapable of grief, or the death is associated with stigma, such as a result of self-harm, suicide, or substance use. Other examples include loss of a terminated pregnancy or a former spouse. Because this type of grief lacks social recognition and customary rituals, individuals are at increased risk for unresolved or complicated grief, making recognition and validation by health care professionals, particularly nurses, essential for providing appropriate emotional support. Ambiguous loss is a specific type of disenfranchised grief in which the person is still physically present but not psychologically present, such as an individual with dementia or traumatic brain injury. Another example of ambiguous loss is when a person is believed to be dead, but no body is found, leaving the loss unresolved and uncertain. This uncertainty prevents closure, often causing prolonged distress because loved ones must grieve while still holding on to hope that the person may be alive (Potter et al., 2026, p. 787).
Nursing Grief and Loss
The nurse is a dedicated caregiver trained to provide physical, emotional, and psychological care to the patient and family. Nurses care for patients through all stages of their illness and treatment, which leads to the restoration of health or the death of the patient. When death is possible, nurses strive to help patients and families empathetically come to terms with the impact of their illness, discuss wishes, set realistic care goals, and make appropriate EOL decisions (ANA, 2024a). For nurses, each connection formed during this period will be accompanied by a subsequent loss once the patient dies. The toll and impact of this loss on the nurse can vary tremendously and is primarily grounded in the nurse’s unique perspectives on death, beliefs, values, prior experiences with death, and several nursing-related factors. Some of the most prominent nursing-related factors that contribute to the grief response in nurses include the clinical practice subspecialty, the amount of exposure to patient death and dying in the workplace, the perceived comfort and skillset providing care for patients and communicating with families at the EOL, and how the death ensues. Oncology, palliative, and hospice nurses are exposed to death and dying much more frequently than nurses in other specialties (e.g., orthopedics or labor and delivery). Therefore, experienced oncology, palliative, and hospice nurses are often at greater ease communicating with patients and families about their care goals, including EOL care, advanced directives, and managing expectations surrounding the dying process. ICU and emergency room (ER) nurses are exposed to death in a manner that is dramatically different from those nurses practicing in oncology or hospice settings, as death may ensue rapidly and without warning. Families may be unprepared, and death is often more traumatic if the care goals are not discussed beforehand. Furthermore, evidence demonstrates that the details surrounding the death experience (i.e., traumatic with several life-prolonging interventions versus an expected death with comfort care measures) can directly impact the nurse’s emotional response and subsequent grieving process (Potter et al., 2026, Chapter 36).
How Grief Can Manifest in Nurses
Across many practice settings, when a patient dies, nurses may experience strong emotional reactions and grief; however, these responses are often unacknowledged or minimized in clinical environments. Unresolved or disenfranchised grief is common among nurses, as they frequently lack the time or opportunity to process the loss of a patient before continuing to care for others. Nurses often develop conscious and subconscious coping strategies, such as emotional distancing or compartmentalization, to manage the death of a patient and maintain their ability to provide supportive care to remaining patients. Nurses commonly continue working despite personal grief, particularly as they serve as a primary source of support for bereaved families in the immediate postdeath period. Persistently suppressing emotional responses related to patient death can create a cumulative burden over time. In addition to limiting opportunities for personal grief, nurses may withhold compassion from themselves, sometimes influenced by the misconception that effective nursing requires emotional toughness or "thick skin." Over time, unresolved grief may contribute to a range of emotional, cognitive, psychological, and physical consequences. These can include emotional and physical exhaustion, moral distress, difficulty concentrating, decreased job satisfaction, depersonalization, burnout, and compassion fatigue (Nantsupawat et al., 2023; Owens et al., 2025; Potter et al., 2026, p. 7).
Compassion fatigue is a broadly defined concept that is well-cited in nursing. Compassion fatigue is characterized by the physical, emotional, and spiritual exhaustion and distress that result from caring for patients and long-term exposure to recurrent human suffering and death, such as nurses caring for patients dying of COVID-19 in ICUs during the height of the pandemic. It can manifest as various physical, emotional, spiritual, and psychological health ailments and induce interpersonal and psychosocial problems. Compassion fatigue is commonly associated with a reduced capacity to provide compassionate care and may involve depersonalization of care. This leads to a decline in the quality of patient care, job dissatisfaction, decreased morale, and burnout. Unaddressed emotional distress and grief can lead to reduced productivity in the workplace through increased absenteeism and increased staff turnover; this has a ripple effect on the remaining staff, who need to absorb the impact of fewer nurses. Further, these consequences fuel a rise in health care costs to the institution and society and contribute to the overall nursing shortage (Gustafsson & Hemberg, 2022; Potter et al., 2026, p. 814).
Moral distress is closely related to compassion fatigue and frequently cooccurs with it in nursing practice. Moral distress encompasses the anxiety, tension, and emotional responses that result from repeated loss and prolonged exposure to patient suffering, specifically in response to personal beliefs and values that conflict with the circumstances surrounding the patient’s care. Ethical issues at the EOL are a significant source of moral distress among nurses; this includes the continued delivery of aggressive interventions to dying patients despite minimal or no clinical benefit, as well as decisions to withdraw life-prolonging or potentially curative therapies. These responsibilities can heighten stress and trigger feelings of powerlessness, hopelessness, and vulnerability (Potter et al., 2026, pp. 323–324; Sheppard et al., 2022).
Emotionally exhausted caregivers may experience symptoms similar to posttraumatic stress disorder, such as recurrent recollections, distressing dreams, and anxiety. Unresolved grief in nurses is associated with reduced cognitive ability, increased risk of medication errors, and impaired clinical judgment. Feelings of isolation, anger, and guilt can develop, in addition to a loss of self-worth and purpose. Some additional signs of declining physical and mental health may include behavioral changes and mood swings. These may be observed by peers and, at times, by patients, potentially contributing to dissatisfaction with care. Nurses may appear lethargic, disinterested in patient care, delayed in response to patient needs, or neglectful of responsibilities. They may become more vocal about job dissatisfaction, complain about patient assignments, or disengage in unit-based activities and committees. These changes can also affect one’s personal life as acknowledged by family and friends and present as increased conflict, arguing, and irritability with close contacts, or by disinterest, withdrawal, or not spending time with loved ones. Dietary and physical activity patterns may change, such as decreased physical activity, changes in eating patterns, and neglect of personal health. In extreme cases, nurses may be at increased risk for maladaptive coping behaviors, including substance misuse (Alshammari et al., 2025; Hostiuc & Gherghiceanu, 2026; Zhang et al., 2024).
The nursing environment, expectations surrounding death, and the type of death also contribute to the severity of the nurse’s grief. Certain nursing specialties care for patients for an extended period through the continuum of their disease process (e.g., oncology, hospice, palliative, and dialysis). There is abundant literature dedicated to grieving patient loss among dialysis and oncology nurses, who regularly care for patients for weeks, months, or even years. Over time, caring relationships are fostered by nurses, generating strong emotional bonds and attachments between the nurse and the patient and family. This can make the patient’s death feel like a personal loss to the nurse. Repeated encounters with patients who are suffering or dying can make grieving more complex and remind nurses of their own mortality or the mortality of their loved ones. Several sources cite that grieving patient loss in ICU settings is often discouraged or unacknowledged due to professional norms and the short duration of caregiving relationships. However, when patient outcomes are less than expected, it can contribute to threats to self-image or professional identity for the nurse (Binoy, 2026; Massey et al., 2025; Tang et al., 2025; Vallone et al., 2025).
Grieving Bad Deaths
The concept of a good death gained prominence alongside the development of the hospice and palliative care movements. Although the term has etymological roots in the word euthanasia, which means "good death," it evolved to represent a distinct philosophy focused on comfort, dignity, and quality of life rather than the deliberate hastening of death (Harmman & Walling, 2025; Oxford Public International Law, 2020). While the idea of what constitutes a good death is different based on social and cultural norms, nurses and other direct health care professionals typically describe a death as good when it is physically comfortable, emotionally and spiritually supported, and grounded in respect and dignity. The patient and family are aware of and prepared for the approaching death and perceive their needs as being met. Care aligns with the patient’s wishes, and the patient is supported by loved ones in a peaceful environment. In contrast, bad deaths are commonly characterized by physical suffering, social isolation, psychological and emotional distress, and care that is discordant with the preferences of the patient and family. Such deaths can be more difficult to grieve, as they disrupt expectations of a peaceful and meaningful EOL experience and may prevent important conversations, resolution of unfinished matters, or a sense of closure. Nurses who witness these deaths may encounter profound human suffering and pain and, over time, may internalize these experiences, contributing to distress and heightened fears related to death, dying, and suffering (Harmman & Walling, 2025; Yu, 2023).
Strategies for Coping With Death and Grief
Unaddressed grief has severe consequences and is more complex for nurses who lack the proper skill set, training, knowledge, attitudes, and support system to facilitate healthy coping. Nurses who lack the coping skills to effectively manage patient death may be inadequate in supporting dying patients and their family members. Nurses who recognize and confront their feelings and reactions to death can develop healthier coping skills and provide higher quality care and support to their patients. In addition, nurses who allow themselves to go through the grieving process are healthier overall and lead more fulfilling lives and careers. Alternatively, those who do not allow themselves to grieve eventually struggle with sustaining satisfying careers and positive relationships. These nurses may also lose their self-confidence and feel a sense of guilt over losing a patient. They also tend to become more distant and are more reluctant to get close to their patients (Kostka et al., 2021; Sharif et al., 2025).
A critical step in preventing the potential negative consequences of unresolved grief is recognition. Nurses need to take the time to acknowledge each patient’s death. Nurses are better positioned to successfully navigate through grief by developing insight into and awareness of their personal feelings surrounding the death. Nurses are encouraged to acquire a heightened awareness and understanding of their personal beliefs and values surrounding death and their preexisting coping strategies, both the good and the bad. These mindfulness activities can help nurses develop more positive and effective coping skills and ensure that personal beliefs do not negatively impact or influence patient care. The fundamental aspects of coping with patient death include self-care, work–life balance, communication skills, a social support network, and emotional resiliency. Ideally, this set of skills should be introduced during nursing school, so the new graduate nurse is prepared and equipped with strategies to preserve their health and well-being before entering the workplace. Reflective journaling is a self-care strategy that helps nurses process emotional experiences, increase self-awareness, and make meaning of clinical events. Reflective writing supports resilience by reducing emotional burden and stress, thereby helping mitigate burnout and compassion fatigue through intentional reflection and emotional processing (Potter et al., 2026, p. 222, 823; Thornton et al., 2025).
Self-Care
Self-care is a core value of holistic nursing and is a proactive and personalized approach to fostering well-being. It refers to any activity one engages in to promote overall health. Nurses who care for themselves tend to grieve better, endure significantly fewer negative consequences of grief, and have an enhanced capacity to provide compassionate care to patients and families. Nurses must recognize that effective self-care is a continually evolving work-in-progress that should remain a priority in both personal and professional environments. There are numerous evidence-supported ways nurses can engage in self-care, but some of the most well-cited strategies include the following:
- take breaks and time to disconnect periodically, especially during long shifts
- engage in healthy lifestyle choices and behaviors, including adequate sleep/rest, hydration, exercise, and healthy eating habits
- identify ways to rejuvenate well-being, such as through music, yoga, relaxation therapies (mindfulness, meditation, reiki, hot bath, massage)
- engage in enjoyable activities as desired (reading, gardening, socializing, etc.)
- seek support from colleagues, friends, or loved ones
- make time for spiritual or religious practices such as praying, attending religious services, or retreats (ANA, 2024b; Ernstmeyer & Christman, 2024; Williams et al., 2022)
Work–Life Balance
Healthcare providers should strive toward an appropriate work–life balance by establishing and maintaining boundaries within and outside of the workplace:
- invest in meaningful relationships with friends and family
- allow space for non-nursing activities
- take dedicated time away from work
- shed the professional role after the workday
- build and maintain positive and healthy interpersonal relationships within the professional environment and personal life
- manage personal life stressors (ANA, 2024b; Ernstmeyer & Christman, 2024; Williams et al., 2022)
Communication and Social Support
Nurses need to identify social support networks and lean on them when needed. Effective communication skills and social support are critical to fostering healthy grieving. Communication cultivates robust connections within the team. Adapting a workplace environment of “sharing and caring,” with regular debriefing sessions, grief counseling sessions, and support from supervisors and colleagues, is a valuable grieving strategy. Nurses with access to supportive environments to effectively debrief following an arduous clinical experience are better positioned to maintain health and professionalism and are less likely to endure compassion fatigue. Bereavement literature consistently demonstrates that support and understanding from fellow nurse coworkers is a crucial way of effectively coping with loss (Borneman et al., 2026; Feng et al., 2024; Yazdan et al., 2023).
There is a three-step process to facilitate addressing the trauma that can result from caring for dying patients: defusing, debriefing, and follow-up. Defusing should occur on the same day as the event, followed by debriefing a few days later. Debriefing with nursing colleagues following a patient’s death is a commonly used and effective strategy for processing difficult experiences. There are different phases of debriefing, including description or reaction, analysis, and application or summary. Informal debriefing sessions are often perceived by nurses as more accessible and supportive. These informal debriefing sessions allow for mutual support between colleagues, creating a safe environment for processing painful emotions and facilitating open discussion of the distressing events surrounding the loss. These sessions may contribute to emotional processing, growth, and professional resilience. Informal debriefing with coworkers may feel more validating for nurses than support from family members. Many feel their family members often cannot fully comprehend or understand their experiences and cannot provide sufficient acknowledgment or validation of their loss. In addition, some nurses find it meaningful to grieve with the family through crying, prayer, or attending the patient’s funeral or memorial services. Follow-up should ensure that the nurse is coping effectively and suggest professional help if needed (DeSpelder et al., 2020; Knott et al., 2023).
Emotional Resiliency
Emotional resiliency is at the core of coping with death and grief and is an important protective factor against compassion fatigue, emotional exhaustion, burnout, and disenfranchised grief in nurses. Resilience is an individual’s ability to overcome or adapt to complicated circumstances and function in a challenging environment while preserving health and well-being and fostering personal growth. It refers to the individual’s capacity to respond to the pressure and demands of daily life and is a survival skill. Some people are innately more resilient than others, and some develop resiliency over time through hardship and life experiences. Factors that promote resiliency include positive social relationships, hope, optimism, spirituality, organizational support, self-efficacy, and having a resilient role model. By maintaining emotional resiliency, nurses are better equipped to provide the best care for themselves and others experiencing grief. Moral distress is a significant predictor of nursing burnout, as there is a strong association between burnout and those with low levels of resilience. A higher level of resiliency protects nurses from emotional exhaustion and is associated with increased hope and reduced stress, burnout, and compassion fatigue, and contributes to heightened personal accomplishment. Correspondingly, nurses with low emotional resilience experience more compassion fatigue and job dissatisfaction (ANA, 2024b; Andersen et al., 2021; Ernstmeyer & Christman, 2024).
Self-care factors such as work–life balance, control, maintaining hope, a sense of professional identity, and perceived emotional support contribute to nurses’ resilience. Higher resilience levels are linked to enhanced self-efficacy, coping, and competence. The ability to cope effectively with pressure, trauma, and uncertainty is premised on underlying behaviors, thoughts, and actions. Many strategies that promote emotional resiliency are also firmly grounded in self-care principles. Some of the most effective ways to build emotional resiliency include the following:
- talking to a trusted confidant
- advocating for personal needs and accepting support
- openly articulating thoughts and emotions
- utilizing Employee Assistance Programs (EAPs) if available
- practicing self-care (as discussed earlier)
- avoiding social media and the news (ANA, 2024b; Potter et al., 2026, p. 823)
Persistent challenges within the US healthcare system place significant strain on nurses, contributing to rising levels of burnout, emotional distress, and moral distress. The Health Care Professional Well-Being Toolkit, developed by CAPC, offers resources to help nurses and other health care professionals support their well-being amid these ongoing pressures. Although nurses need to take responsibility for developing effective personal strategies to manage grief and facilitate successful coping and emotional resiliency, organizational support is also an integral element in helping nurses cope with loss. Leaders are encouraged to engage in advocacy and system-level initiatives to create lasting change in the US healthcare environment (CAPC, 2024). Unfortunately, loss and bereavement remain insufficiently addressed across health care settings. There remains a lack of emotional support and resources consistently available to nurses when patients die, even in the oncology and hospice fields, where death is commonplace. Lack of employer support in acknowledging and dealing with patient loss, grief, and bereavement is a recurrent theme across the literature. Health care administrators and nurse leaders are fundamental to the early identification of nurses at risk for compassion fatigue and complicated grief. Developing and implementing bereavement programs designed explicitly for nurses can provide the time, environment, and skills training to channel emotions surrounding patient death in a healthy manner. Leaders can contribute to a reduction in burnout, turnover risk, and compassion fatigue and enhance job satisfaction by generating a supportive environment and educating on recognizing and adequately managing personal bereavement. Strategies proposed in the literature include the following:
- monthly grief rounds to provide regular, structured opportunities for reflection and shared processing
- facilitated discussion groups that support emotional expression through remembrance activities, debriefings, retreats, counseling, and pastoral care
- peer support or mentorship programs that offer confidential emotional support from trained colleagues
- protected time for postdeath pauses or rituals to acknowledge loss and allow brief reflection following a patient’s death
- integration of palliative care consultation to support staff through interdisciplinary debriefing and emotional guidance
- staff training through bereavement care services to develop coping skills, communication strategies, and healthy grief processing
- group processing activities such as writing, storytelling, journaling, or the use of memory boards to promote meaning-making
- skills-based training programs focused on building resilience, compassion, and effective self-care practices
- supportive workplace interventions including adequate breaks, time off, and thoughtful adjustment of patient care assignments (Borneman et al., 2026; Reinken & Rizek, 2025; Soper, 2022; Yazdan et al., 2023)
References
Alshammari, S. A., Sankarapandian, C., Pasay an, E., Alshammary, A. A., Gonzales, A., Gutierrez, J., Alreshidi, M. S., Alrashidi, N. A., Pangket, P., Cabansag, D., Alkubati, S., Mostoles, R., Lagura, G. A., Albarak, S. H., & Saguban, R. (2025). A predictive study of factors associated with burnout, compassion fatigue, and moral distress among emergency nurses. Scientific Reports, 15(1), 30596. https://doi.org/10.1038/s41598-025-14792-5
American Nurses Association. (2024a). Nurses' roles and responsibilities in providing care and support at the end of life. https://www.nursingworld.org/globalassets/docs/ana/practice/official-position-statements/nursesrolesandresponsibilitiesinprovidingcareandsupportattheendoflife_revised_bod-approved_final.pdf
American Nurses Association. (2024b). Three steps to build resilience. Retrieved April 28, 2026, from https://www.nursingworld.org/content-hub/resources/nursing-leadership/three-steps-to-build-resilience/
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders: DSM-5-TR (5th ed.). Author.
American Psychiatric Association. (2025). Prolonged grief disorder. https://www.psychiatry.org/patients-families/prolonged-grief-disorder
Andersen, S., Mintz-Binder, R., Sweatt, L., & Song, H. (2021). Building nurse resilience in the workplace. Applied Nursing Research, 59, 151433. https://doi.org/10.1016/j.apnr.2021.151433
Binoy, S. J. (2026). Grief and coping strategies among hematology-oncology nurses: An integrative review. Athens Journal of Health and Medical Sciences, 13(1), 47–66. https://doi.org/10.30958/ajhms.13-1-3
Borneman, T., Hayward, P., & Buller, H. (2026). Bereavement support for oncology nurses caring for patients and families. Journal of Hospice and Palliative Nursing, 28(2), 84–93. https://doi.org/10.1097/NJH.0000000000001180
Center to Advance Palliative Care. (n.d.). About palliative care. Retrieved April 28, 2026, from https://www.capc.org/about/palliative-care
Center to Advance Palliative Care. (2024). Health care professional well-being. Retrieved April 28, 2026, from https://www.capc.org/toolkits/health-care-professional-well-being/
DeSpelder, L. A., Stickland, A. L., Potts, J. M., & Mason, M. (2020). The last dance: Encountering death and dying (11th ed.). McGraw Hill.
Ernstmeyer, K., & Christman, E. (Eds.). (2024). Nursing management and professional concepts (2nd ed.). Chippewa Valley Technical College. https://www.ncbi.nlm.nih.gov/books/NBK610441/
Feng, H., Shen, Y., & Li, X. (2024). Bereavement coping strategies among healthcare professionals: A qualitative systematic review and meta-synthesis. Palliative & Supportive Care, 22(6), 2194–2206. https://doi.org/10.1017/S1478951524001147
Freud, S. (1917). Mourning and melancholia. Metapsychology, IV, 152–170. http://www.columbia.edu/itc/hs/medical/clerkships/psych/misc/articles/freud.pdf
Gustafsson, T., & Hemberg, J. (2022). Compassion fatigue as bruises in the soul: A qualitative study on nurses. Nursing Ethics, 29(1), 157–170. https://doi.org/10.1177/09697330211003215
Harmman, S. M., & Walling, A. M. (2025). Palliative care: The last hours and days of life. UpToDate. Retrieved April 28, 2026, from https://www.uptodate.com/contents/palliative-care-the-last-hours-and-days-of-life
Hostiuc, S., & Gherghiceanu, F. (2026). Burnout, PTSD, and medical error: The medico-legal implications of the mental health crisis among frontline healthcare professionals during COVID-19. Medicina, 62(2), 305. https://doi.org/10.3390/medicina62020305
Knott, H., Dambrino, K. L., Busby, S., & Rasmussen, A. (2023). Debriefing among hospice professionals during a pandemic. Journal of Hospice & Palliative Nursing, 25(2), 90–96. https://doi.org/10.1097/NJH.0000000000000930
Kostka, A. M., Borodzicz, A., & Krzemińska, S. A. (2021). Feelings and emotions of nurses related to dying and death of patients—A pilot study. Psychology Research and Behavior Management, 14, 705–717. https://doi.org/10.2147/PRBM.S311996
Massey, C. C., Conway, J., & Webster, E. (2025). Bereavement in haemodialysis units: A scoping review of the perspectives and experiences of patients and nursing staff and support strategies. BMJ Open, 15(10), e104382. https://doi.org/10.1136/bmjopen-2025-104382
Meier, D. E., McCormick, E., & Lagman, R. L. (2025). Hospice: Philosophy of care and appropriate utilization in the United States. UpToDate. Retrieved April 28, 2026, from https://www.uptodate.com/contents/hospice-philosophy-of-care-and-appropriate-utilization-in-the-united-states
Nantsupawat, A., Wichaikhum, O., Abhicharttibutra, K., Sadarangani, T., & Poghosyan, L. (2023). The relationship between nurse burnout, missed nursing care, and care quality following COVID‐19 pandemic. Journal of Clinical Nursing, 32(15–16), 5076–5083. https://doi.org/10.1111/jocn.16761
National Cancer Institute. (n.d.). End-of-life care. Retrieved April 28, 2026, from https://www.cancer.gov/publications/dictionaries/cancer-terms/def/end-of-life-care
National Cancer Institute. (2024). Grief, bereavement, and coping with loss (PDQ®)—Health professional version. https://www.ncbi.nlm.nih.gov/books/NBK66052
Owens, D., Morse, R., Garcia-Greenwood, L., Daly, C., & Phan, T. M. (2025). Understanding disenfranchised grief in a post-COVID-19 world—A pilot study of advanced practice registered nurses in palliative care. Journal of Hospice and Palliative Nursing, 27(1), E17–E26. https://doi.org/10.1097/NJH.0000000000001079
Oxford Public International Law. (2020). Euthanasia. Retrieved April 28, 2026, from https://opil.ouplaw.com/display/10.1093/law:epil/9780199231690/law-9780199231690-e793
Potter, P. A., Perry, A. G., Stockert, P. A., Hall, A. M, & Ostendorf, W. R. (2026). Fundamentals of nursing (12th ed.). Elsevier.
Prigerson, H. G., Singer, J., & Killikelly, C. (2024). Prolonged grief disorder: Addressing misconceptions with evidence. The American Journal of Geriatric Psychiatry, 32(5), 527–534. https://doi.org/10.1016/j.jagp.2023.10.020
Reinken, D. N., & Rizek, J. (2025). Strategies to prevent and effectively respond to compassion fatigue and burnout. Journal of Emergency Nursing, 51(2), 205–210. https://doi.org/10.1016/j.jen.2024.10.004
Schoo, C., Azhar, Y., Mughal, S., & Rout, P. (2025). Grief and prolonged grief disorder. In StatPearls [Internet]. StatPearls Publishing. Retrieved April 28, 2026, from https://www.ncbi.nlm.nih.gov/books/NBK507832
Sharif, L., Almutairi, K., Alnasser, I., Attar, Z., Mahsoon, A., Alhofaian, A., Almutairi, B., Alqahtani, Y., Tunsi, A., Yaghmour, S., Bokhari, F., & Wright, R. (2025). Relationship between grief and coping strategies among nurses dealing with patient deaths: a descriptive, cross-sectional, correlational study. BMC Palliative Care, 24(1), 151. https://doi.org/10.1186/s12904-025-01790-7
Shear, M. K., Reynolds, C. F., Simon, N. M., & Zisook, S. (2026). Bereavement and grief in adults: Clinical features. UpToDate. Retrieved April 28, 2026, from https://www.uptodate.com/contents/bereavement-and-grief-in-adults-clinical-features
Sheppard, K. N., Runk, B. G., Maduro, R. S., Fancher, M., Mayo, A. N., Wilmoth, D. D., Morgan, M. K., & Zimbro, K. S. (2022). Nursing moral distress and intent to leave employment during the COVID-19 pandemic. Journal of Nursing Care Quality, 37(1), 28–34. https://doi.org/10.1097/NCQ.0000000000000596
Soper, K. (2022). Reducing burnout and promoting professional development in the palliative care service. Journal of Hospice & Palliative Nursing, 24(3), 181–185. https://doi.org/10.1097/NJH.0000000000000847
Tang, T., Yang, J., Wang, C., Zou, Y., & Liu, Y. (2025). Key enablers and barriers to ICU nurses’ professional identity: A qualitative study. Frontiers in Medicine, 12, 1695617. https://doi.org/10.3389/fmed.2025.1695617
Thornton, E., Moseley, L., Noll, K., & Lambert, A. W. (2025). Recognizing grace in grief through reflection in nursing education: A qualitative research study. Journal of Hospice and Palliative Nursing, 27(2), 81–86. https://doi.org/10.1097/NJH.0000000000001094
Tyrrell, P., Harberger, S., & Siddiqui, W. (2023). Kubler-Ross stages of dying and subsequent models of grief. In StatPearls [Internet]. StatPearls Publishing. Retrieved April 28, 2026, from https://www.ncbi.nlm.nih.gov/books/NBK507885
Vallone, F., Lambiase, C. V., & Zurlo, M. C. (2025). The psychological impact of dealing with death and the risk of dying among nurses working in ICU and NICU: Specificities in mediating and moderating variables. Healthcare (Basel), 13(18), 2265. https://doi.org/10.3390/healthcare13182265
Yarbro, C. H., Wujcik, D., & Gobel, B. H. (2018). Cancer nursing: Principles and practice (8th ed.). Jones and Bartlett Publishers.
Williams, S. G., Fruh, S., Barinas, J. L., & Graves, R. J. (2022). Self-care in nurses. Journal of Radiology Nursing, 41(1), 22–27. https://doi.org/10.1016/j.jradnu.2021.11.001
World Health Organization. (2023). Palliative care. https://www.who.int/europe/news-room/fact-sheets/item/palliative-care
Yazdan, R., Corey, K., Messer, S. J., Kim, E. H., Roberts, K. E., Selwyn, P. A., & Weinberger, A. H. (2023). Hospital-based interventions to address provider grief: A narrative review. Journal of Pain and Symptom Management, 66(1), e85–e107. https://doi.org/10.1016/j.jpainsymman.2023.03.001
Yu, T. (2023). A ‘Good’ Death. Journal of Brown Hospital Medicine, 2(1), 66289. https://doi.org/10.56305/001c.66289
Zhang, Z., Gao, M., Fang, Z., Chen, X., Shen, Q., & Gao, Y. (2024). The coping strategies and cumulative changes in intensive care unit nurses after experiencing professional grief: A hermeneutic phenomenological study. Journal of Nursing Management, 3682609. https://doi.org/10.1155/2024/3682609
Powered by Froala Editor