This course examines the safe and effective use of medical cannabis and cannabinoids, outlining the various medicinal benefits and pertinent prescribing information to safeguard patient care, improve outcomes, and uphold the practice of the advanced practice registered nurse (APRN).
...purchase below to continue the course
ment, added to a food, or marketed with claims of preventing, diagnosing, treating, or curing a serious disease, such as cancer. The FDA may pursue enforcement action when a product violates the FD&C Act, specifically if it threatens public health (FDA, 2024).
In 2015, the US Department of Health and Human Services (2015) announced that it would no longer require nonfederally funded cannabis studies to be vetted and approved by the Public Health Service (PHS), removing a hurdle and helping to facilitate further research. As more states pass laws legalizing cannabis for recreational use, the number of Americans supporting its use for medical purposes continues to increase. The Pew Research Center (2024) found that 57% of Americans polled support the legalization of cannabis for medical and recreational purposes, while 32% support legalization for medical use only, and only 11% of Americans believe it should not be legal. Despite this public approval, state and federal laws are conflicting. While many states have enacted laws and policies allowing use of cannabis for medical and recreational purposes, these activities still violate the Controlled Substances Act, which still classifies cannabis as a schedule I controlled substance. In 2024, the US Department of Justice (DOJ) formally submitted a proposal to reclassify cannabis from a schedule I to a schedule III substance under the Controlled Substances Act, acknowledging its accepted medical use and lower misuse potential (DOJ, 2024). Moving cannabis to a schedule III substance would theoretically allow it to be used for medical purposes; however, schedule III substances require a valid prescription, and cannabis is currently not an approved prescription drug by the FDA. Due to the conflict between state-level legalization and federal prohibition, individual prescribers continue to express concerns about the potential threat to their federal DEA registration status. Hospitals also remain reluctant to embrace cannabinoid treatments for fear of losing federal Medicare/Medicaid funding. In 2025, an executive order was signed, which directs federal agencies to accelerate the process of reclassifying cannabis from a schedule I to schedule III substance, recognizing its potential for medical use (Cheng et al., 2022; Sheikh, 2026; The White House, 2025; Zammit Dimech et al., 2025).
California was the first to legalize medical cannabis use with Proposition 215 in 1996. Currently, 40 states, as well as the District of Columbia, Guam, Puerto Rico, and the US Virgin Islands, allow the medical use of cannabis products. In addition, approved measures in eight states allow the use of “low THC, high CBD” products for medical reasons in specific situations, as shown in Figure 1. Low-THC programs are not counted as comprehensive medical cannabis programs. As of June 2025, 24 states, three territories, and the District of Columbia have legalized or regulated recreational use of cannabis by adults without medical certification (National Conference of State Legislatures [NCSL], 2025). There are no public access programs currently available in Idaho and Kansas. The Agriculture Improvement Act of 2018 removed hemp from the federal Controlled Substances Act, which means that cannabis plants and derivatives that contain no more than 0.3% of THC on a dry weight basis are no longer controlled substances under federal law (FDA, 2024). The updated definition in 2025 included total THC concentration, not just the delta-9 THC (Neuhofer et al., 2025). Refer to Figure 1 from the NCSL website. Cannabis use is also legal for adult use in Canada and parts of Europe (NCSL, 2025).
Figure 1
State-Regulated Cannabis Programs
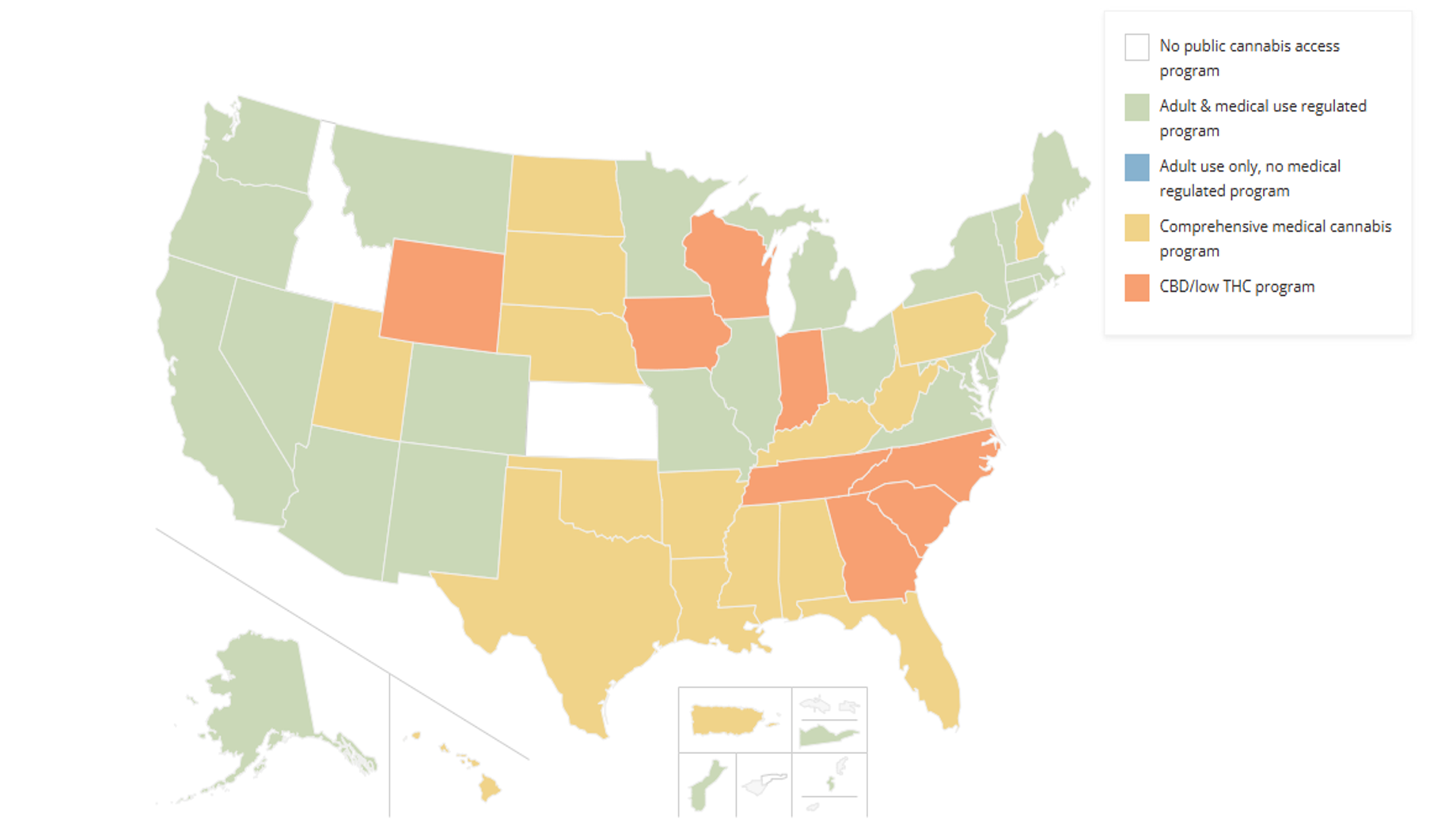
(NCSL, 2025)
FDA Approvals
There are many types of synthetic cannabinoids that are manufactured and sold, though many are banned by the US federal government. Synthetic or purified cannabinoids act on the same receptors in the brain as endogenous cannabinoids. They can be administered by smoking, vaping through electronic delivery devices (i.e., cannabis pens, e-pens, or vaporizers), or ingested in herbal tea or food. The FDA has only approved three synthetic THC formulations (nabilone [Cesamet], dronabinol [Marinol] capsule, dronabinol [Syndros] oral solution) and one cannabis-derived drug product, CBD (Epidiolex). These products are only available with a prescription from a licensed HCP. Nabilone (Cesamet) is a schedule II capsule currently approved by the FDA to treat nausea and vomiting associated with cancer chemotherapy in patients who have failed to respond to conventional antiemetic treatments. Dronabinol is a schedule III medication available in capsule form (Marinol) and oral solution (Syndros). Both are FDA-approved to treat nausea and vomiting related to chemotherapy after failure to respond to conventional antiemetic treatments and for treating anorexia and weight loss in patients with HIV/AIDs. Before prescribing these medications, HCPs are encouraged to assess the patient’s risk for substance use or misuse. These agents may induce psychiatric and cognitive effects impairing mental or physical abilities. Those with a history of substance misuse, dependence, or psychiatric history are at heightened risk for misuse and adverse effects (FDA, 2023, 2024; NCSL, 2025; Patel et al., 2024; Slawek & Arnsten, 2025).
In 2018, the FDA approved CBD (Epidiolex) for treating seizures in patients 2 years and older associated with two severe forms of epilepsy, Lennox-Gastaut syndrome (LGS) and Dravet syndrome. Both conditions are rare, appear early in life, and can cause difficult-to-control and potentially life-threatening seizures. Cannabidiol (Epidiolex) is the first FDA-approved drug containing a purified substance derived from cannabis. The efficacy of CBD (Epidiolex) was evaluated through three randomized, double-blind, placebo-controlled clinical trials involving 516 patients with either LGS or Dravet syndrome. Within these studies, when CBD (Epidiolex) was taken alongside other medications, it reduced the frequency of seizures compared to a placebo. The most common side effects include sedation, sleepiness, fatigue, weakness, malaise, and lethargy. Less common side effects include elevated liver enzymes, decreased appetite, diarrhea, skin rash, and insomnia. Aside from CBD (Epidiolex), no other FDA-approved drug products contain CBD. Outside of the United States (Canada and Europe), nabiximols (Sativex) is a purified natural combination that includes equal parts of THC and CBD in an oromucosal spray formulation for the treatment of pain and spasticity (FDA, 2023; Patel et al., 2024; Schachter & Sirven, 2026; Slawek & Arnsten, 2025).
Medicinal Uses
In 2020, the United Nations officially recognized the medical value of cannabinoids for treating many different diseases. Since this time, there has been a growing interest in research to establish the effectiveness of cannabinoids for various diseases. Bilbao and Spanagel (2022) conducted a systematic review and meta-analysis of medical cannabinoids for efficacy, retention, and adverse effects to help establish the grade of evidence available to inform policy and clinical decisions. Bilbao and Spanagel (2022) acknowledge that previous reviews were limited in their coverage of various diseases and did not consider that medical cannabinoids account for plant-derived and synthetic derivatives, which differ in their pharmacology. The researchers identified 6,308 abstracts, narrowed to 152 randomized controlled trials (RCTs), with 53 evaluating dronabinol (Marinol, Syndros), 35 nabilone (Cesamet), 27 CBD, and 37 nabiximols (Sativex). The researchers found that CBD had a significant therapeutic effect on seizure disorders (standardized mean difference [SMD] −0.5 [95% CI −0.62 to −0.38]; high grade) and Parkinsonism (−0.41 [95% CI −0.75 to −0.08]; moderate grade). Moderate evidence was found for the use of dronabinol (Marinol, Syndros) for appetite stimulation −0.51 (95% CI −0.87 to −0.15), chronic pain −0.31 (95% CI −0.46 to −0.15), and Tourette syndrome −1.01 (95% CI −1.58 to −0.44). In addition, moderate evidence was also found for the use of nabiximols (Sativex) for spasticity −0.36 (95% CI −0.54 to .19), sleep −0.24 (95% CI −0.35 to −0.14), chronic pain −0.25 (95% CI −0.37 to −0.14), and substance use disorder (SUD) −0.48 (95% CI −0.92 to −0.04). The remaining studies showing a significant therapeutic effect were grade low, very low, or no grade evidence. The researchers concluded that additional research and systematic reviews are needed (Bilbao & Spanagel, 2022).
In a 2018 Cochrane systematic review of cannabis-based medicine on neuropathic pain in adults, the researchers found 16 studies with 1,750 patients. Specifically, the researchers wanted to assess the efficacy, tolerability, and safety of cannabis-based medicines (i.e., synthetic, plant-derived, or herbal) compared to placebo or conventional drugs for the treatment of neuropathic pain in adults. The researchers found an increase in the number of patients achieving 50% or greater pain relief from the cannabis-based medicine (21%) compared to the placebo (17%). However, the quality of evidence was determined to be low (Mücke et al., 2018). In addition, Mücke and colleagues (2018) found that more participants withdrew due to adverse events in the cannabis-based medicines versus the placebo. They determined that there was insufficient evidence to determine if cannabis-based medicines increase the frequency of serious adverse events. Finally, psychiatric disorders occurred in 17% of participants in the cannabis-based medicines group versus 5% in the placebo group. The researchers concluded that the minor improvements in neuropathic pain might outweigh the potential harm; however, more research is needed (Mücke et al., 2018). Bell and colleagues (2024) evaluated the use of cannabinoid-based medicines (CBM) for the management of chronic pain. They reviewed over 70 articles and found a moderate benefit of CBM on chronic pain management. In addition, there was also evidence that demonstrated that CBM was effective in the management of comorbidities such as anxiety, appetite suppression, and sleep problems (Bell et al., 2024).
In 2022, Haddad and colleagues evaluated the efficacy of cannabis on multiple sclerosis (MS)-related symptoms. The oromucosal spray nabiximols (Sativex) and oral cannabinoids were found to improve spasticity and pain related to MS but were less effective in other MS-related symptoms. Similarly, Filippini and colleagues (2022) conducted a systematic review and meta-analysis to assess the benefit and harm of cannabinoids in reducing symptoms of MS. The researchers found 25 RCTs, with 3,763 participants, including 2,290 who received cannabinoids. Filippini and colleagues (2022) found that nabiximols (Sativex) probably increased the number of people with perceived reductions in spasticity compared to placebo, moderate-quality evidence. In addition, the researchers found that evidence for neuropathic pain associated with MS is of very low quality, making it difficult to determine whether there is reduced chronic pain. AlHabil and colleagues (2026) conducted a systematic review and meta-analysis evaluating the role of cannabis in managing spasticity in MS. They included nine clinical trials and determined that there was a notable improvement in spasticity scores, particularly over a longer duration for individuals taking cannabis; however, they caution that despite these promising findings, they noted elevated heterogeneity across studies. They recommend future high-quality studies with standardized protocols to evaluate long-term outcomes. Despite some of these positive findings, there is currently no evidence that medical cannabis has an overall effect on slowing the progression of MS. Nabiximols (Sativex) is approved in Canada and other countries for the treatment of neuropathic pain due to MS, but is not currently approved in the United States (Hesketh, 2024).
As previously stated, cannabis and cannabinoid use in treating epilepsy has also been studied, particularly in special populations of pediatric refractory epilepsy syndromes that tend to respond poorly to traditional antiseizure drugs. The American Academy of Neurology and Cochrane reviews completed in 2014 rated the evidence for cannabis use in treating epilepsy as limited, inconclusive, or insufficient. Mouhamed and colleagues (2018) assessed treatment with THC as too broad for therapeutic purposes. However, they found positive findings when they reviewed five trials published between 2013 and 2018 studying the use of CBD in treating drug-resistant epilepsy in children or young adults (three of which were referenced above in the section on CBD [Epidiolex]). These studies showed a more significant reduction in the frequency of atonic and partial seizures, followed by reductions in tonic/tonic-clonic seizures, with minimal reports of adverse effects. Of note, these studies did not utilize CBD as a replacement for the subjects’ antiseizure medications but as an adjunct. More recent studies have confirmed the effectiveness of CBD (Epidiolex) in children and adults with treatment-resistant epilepsy. In a 2018 study of 607 patients, Szaflarski, Bebin, Comi, and colleagues found that adjunctive use of CBD may have a long-term efficiency for treatment-resistant epilepsy. In another open-label prospective study of 72 children and 60 adults with treatment-resistant epilepsy, CBD (Epidiolex), researchers found a significant reduction in frequency and severity of seizures at 12 weeks sustained over the 48-week duration of treatment (Szaflarski, Bebin, Cutter, et al., 2018).
Mouhamed and colleagues (2018) found that studies including patients with posttraumatic stress disorder (PTSD) showed consistently decreased frequency of nightmares when treated with nabilone (Cesamet) or 5 mg THC in oil, and several case reports of decreased tic severity and frequency in patients with TS when given CBD/THC daily. Stanciu and colleagues (2021) conducted a systematic review to evaluate the effectiveness of cannabinoids in the treatment of mood disorders, anxiety, and PTSD. They found only eight very small studies with inconsistent findings and, therefore, insufficient evidence to recommend cannabinoids for the treatment of mood disorders, anxiety, or PTSD. Another systematic review conducted by Urbi and colleagues (2022) evaluated the effect of cannabis in Parkinson’s disease. The researchers included 23 studies, five of which were randomized controlled trials, and found that there was not a clinically significant improvement in overall Parkinson’s symptoms with the use of cannabis. They did find a potential benefit related to the alleviation of tremors, anxiety, pain, and sleep quality. Further research is needed to determine the benefit of cannabis in the treatment of Parkinson’s disease. When considering cannabinoids in the treatment plan for neurological disorders, it is essential to remember that nearly all of the studies reviewed list anxiety, dysphoria, psychosis, hallucinations, paranoia, and possible perceptual changes as potential adverse effects of cannabinoid products that contain THC (Mouhamed et al., 2018).
Due to CB1 receptors in the GI tract, specific GI effects have been credited to and therapeutically tested in cannabinoids, such as nausea and vomiting. Five studies were reviewed for appetite stimulation and weight gain and compared dronabinol (Marinol, Syndros) with a placebo, megestrol acetate (Megace), or cannabis. Although the measures and endpoints varied, efficacy was only found in one study that showed that dronabinol (Marinol) significantly improved chemosensory perception and other secondary outcomes, including the taste of food, premeal appetite, and the proportion of calories consumed as protein, compared to placebo. Dronabinol (Marinol) was generally well tolerated across studies, regardless of dose or product (Razmovski-Naumovski et al., 2022). Further, megestrol acetate (Megace) is a synthetic progesterone associated with an increased risk for blood clots and cardiac infarction, making it a riskier adjunctive medication in the oncologic setting (Bach, 2025). According to Mouhamed and colleagues (2018), cannabinoid products performed at least as well and sometimes better than ondansetron (Zofran) but had higher rates of adverse effects. Two trials evaluated THC in postoperative nausea and vomiting and found no significant difference compared to the placebo, and unacceptable adverse effects were reported. In patients diagnosed with inflammatory bowel disease (IBD), self-medicating users reported decreased abdominal pain, nausea, diarrhea, joint pain, and increased appetite with cannabis use. However, there is a lack of reliable clinical evidence, as these are the results of self-report observations and are not premised on data compiled from clinical trials. The use of cannabis in IBD patients also correlated with higher rates of surgical procedures, leading the authors to question if cannabis could be masking disease activity and progression (Mouhamed et al., 2018).
The use of dronabinol (Marinol, Syndros) is FDA-approved for the treatment of refractory chemotherapy-induced nausea and vomiting (CINV). Although research has demonstrated moderate benefits of cannabinoids for CINV, the side effects of this treatment can potentially outweigh the benefits, particularly in older adults. Several systematic reviews and meta-analyses have been conducted to evaluate the efficacy of synthetic cannabinoids for the prevention and management of CINV; however, very little data on the effectiveness of inhaled or ingested cannabis has been established (Hesketh, 2024). Allan and colleagues (2018) conducted a systematic review evaluating the effects of cannabinoids on pain, spasticity, and nausea and vomiting, as well as identifying adverse events. The researchers found that there was moderate evidence to support the use of cannabinoids in the treatment of CINV. There was also evidence that individual adverse effects are very common, including dizziness, sedation, confusion, and dissociation, causing some patients to stop treatment. The National Cancer Institute (NCI) reports a beneficial effect of the cannabinoids dronabinol (Marinol, Syndros) and nabilone (Cesamet) when used for CINV but found inconclusive evidence on the use of smoked/inhaled cannabis for CINV (NCI, 2025). According to the American Cancer Society (ACS), there is potential evidence based on in vitro studies that THC and CBD can slow growth and even cause cell death in specific cancer cells. In preclinical trials, cannabinoids reduced the spread of some forms of cancer. Although early clinical trials of cannabinoid use in cancer patients indicate it is safe, they have not established its effectiveness in curing or helping to control the disease (ACS, 2025; Tomko et al., 2020).
Adverse Effects and Patient Counseling
Potential adverse effects of cannabinoids vary greatly depending on the composition of the individual product being evaluated. In epilepsy studies, adverse effects of CBD were reported as fatigue/somnolence, diarrhea, and decreased appetite, while cannabis and THC cause nausea, dizziness, weakness, behavioral/mood changes, hallucinations, suicidal ideations, fatigue, and feelings of intoxication. Anxiety; dysphoria; psychosis; impairment of memory, coordination, judgment, attention, and/or perception; tachycardia, hypertension, increased cardiac output, redness of the conjunctiva, increased appetite, dryness of mouth, and increased risk of being involved in a motor vehicle accident are potential acute adverse effects of THC/cannabis. Chronic use also carries the risk for memory and cognitive deficits, respiratory and immune system effects that increase the risk for infections, airway inflammation and bronchitis, social dysfunction, difficulty in school for adolescents, decreased job performance, increased unemployment, decreased income levels, and decreased satisfaction with life. Although the addiction potential is lower for cannabis than other substances, there does exist a roughly 9% risk for physical/psychological addiction in adults (Patel et al., 2024; Shane-McWhorter, 2025; Slawek & Arnsten, 2025). According to multiple large studies, there does not appear to be a clear epidemiological link between cannabis and lung cancer, as with tobacco users. It remains inconclusive and a topic for further exploration, as “heavy use” of cannabis (more than 50 times in a lifetime) may carry some increased risk of testicular, prostate, or squamous cell carcinomas (NCI, 2025).
As with any treatment plan in medicine, especially one that may include a medication that carries the risk of adverse effects, full disclosure of risks to the patient, extensive counseling, and screening are vital to upholding safety and ensuring positive outcomes. Addiction risk factors include genetic inheritance (at least 50%) and comorbid psychiatric disorders. In adolescents, risk factors include peer usage and academic difficulties in school (Slawek & Arnsten, 2025). When considering whether cannabinoid treatment is appropriate for a particular patient, the patient characteristics listed in Table 1 should be considered.
Table 1
Criteria to Consider When Certifying Cannabinoid Use
- State regulations
- Presence of a qualifying condition
- Interaction with other medications
- Age (extreme caution with patients under 18)
- Severity/nature of the disorder (“debilitating or terminal condition”)
- Prior or current psychiatric or substance use disorder (including a personal or family history of psychosis or cannabis use disorder)
- Failure of standard medical therapies and/or approved cannabinoid products (dronabinol [Marinol, Syndros]/nabilone [Cesamet])
- Underlying cardiac and pulmonary disease
- Agreement to regular follow-up visits
- Acceptance of a detailed explanation of risks, both physical and legal
|
(Buppert & Klein, 2021; Slawek & Arnsten, 2025)
Regarding counseling patients within states that allow the recreational use of cannabis for adults, the American Journal of Public Health developed some evidence-based recommendations for safe cannabis use. These are identified as the Lower-Risk Cannabis Use Guidelines (LRCUGs) and could be utilized by HCPs as a framework for counseling patients who elect to use cannabis recreationally. Their initial recommendations were updated in 2022 and are listed in Table 2; these LRCUGs are intended to reduce the overall risk of adverse effects of cannabis use. However, they are not a guarantee against adverse effects in any particular patient and instead strive to inform patients who may be willing to modify their use to reduce some of the health risks (Fischer et al., 2022).
Table 2
Major Recommendations for Counseling Patients on Cannabis
- There is no universally safe level of cannabis; abstinence is the safest option to avoid harm
- Avoid early age of initiation (before age 16)
- Choose low-potency tetrahydrocannabinol (THC) products or those balanced in cannabidiol (CBD)/THC composition
- All available modes of use have some risk of harm; choose nonsmoking methods/avoid cannabis inhalation
- If using the inhalation mode, avoid deep inhalation
- Avoid high-frequency use (daily or near-daily)
- Use legal and quality-controlled cannabis products and use devices
- If someone experiences impaired cognitive performance, consider temporarily suspending or reducing the intensity (frequency and potency) of cannabis use
- Refrain from driving or operating heavy machinery while using cannabis products
- Individuals who intent to procreate and females who are pregnant or breastfeeding should abstain from cannabis use
- Exercise caution in combining other psychoactive substances with cannabis use
- High-risk populations should avoid use altogether (personal or family history of psychosis or substance use disorder, pregnant individuals)
- Avoid combining the aforementioned high-risk behaviors (such as early age of onset and driving)
|
(Fischer et al., 2022)
HCPs should also be aware that CBD can interact with many medications. CBD is metabolized by the cytochrome p450 (CYP) enzymes CYP3A4 and CYP2C19; coadministration with other medications metabolized or inhibited by CYP3A4 or CYP2C19 can increase or decrease the effectiveness of the medication or the CBD (Shane-McWhorter, 2025; Slawek & Arnsten, 2025). CBD may increase the concentration and effects of the following medications:
- antiseizure medications (e.g., clobazam [Sympazan], topiramate [Topamax], carbamazepine [Tegretol], brivaracetam [Briviact])
- digoxin (Lanoxin)
- fluconazole (Diflucan)
- immunosuppressants (e.g., cyclosporin [Neoral], tacrolimus [Prograf])
- tricyclic antidepressants
- proton pump inhibitors (e.g., omeprazole [Prilosec])
- nicotine
- lithium (Lithobid)
- anticoagulants (e.g., warfarin [Coumadin])
- methadone (Dolophine)
- levothyroxine (Synthroid)
- ketamine (Ketalar; Shane-McWhorter, 2025; Slawek & Arnsten, 2025)
CBD can also cause drowsiness, so caution should be taken if the patient takes other sedatives (e.g., benzodiazepines, alcohol, opioids). Since CBD can cause liver injury, caution should be taken when combined with other hepatotoxic medications, such as acetaminophen (Tylenol) or valproic acid (Depakene, Depacon; Shane-McWhorter, 2025; Slawek & Arnsten, 2025).
Prescriptive Authority
To qualify for a medical use cannabis license, patients must have an authorized HCP to certify that they have a qualifying condition and obtain their license from the state. Medical cannabis patient registries have been devised to monitor these patients as an added layer of regulation; however, the programs are governed by each state, and there is tremendous variation between programs. For instance, California collects minimal or no data in voluntary registries, whereas states like Arizona collect and publish detailed reports. There is also a significant variability between what designates a qualifying patient condition and an authorized prescriber, as these are additionally subjected to state regulations (Centers for Disease Control and Prevention [CDC], 2024). Currently, 18 states and the District of Columbia permit APRNs as providers to certify a patient with a qualifying medical condition to use medical cannabis. According to Act 21-565, Medical Marijuana Omnibus Amendment Act of 2022, this does not confer prescriptive authority, as cannabis is listed as a schedule I controlled substance by the DEA. Instead, designated APRNs in these states have the authority to recommend the use of this substance as described by each state’s law (Haney, 2023). Each state has a list of qualifying medical diagnoses to certify the use of medical cannabis. A few of the most common qualifying conditions are listed in Table 3. However, this list is not comprehensive, and HCPs are encouraged to refer to individual state policies for an accurate list of qualifying diagnoses in the designated state of interest (Buppert & Klein, 2021; Office of Cannabis Management, n.d.; Slawek & Arnsten, 2025).
Table 3
Common Qualifying Medical Conditions for Medical Cannabis Use
- Cancer
- Cachexia
- Glaucoma
- HIV/AIDS
- Hepatitis C
- Amyotrophic lateral sclerosis/Lou Gehrig’s disease
- Parkinson’s disease
- Crohn’s disease
- Posttraumatic stress disorder
- Seizures/epilepsy
|
(Office of Cannabis Management, n.d.; Slawek & Arnsten, 2025)
The American Nurses Association (ANA) has openly supported the use of medical cannabis since 1996. In a 2021 reaffirmed position statement, the ANA supports reviewing and reclassifying cannabis’s status as a schedule I drug under federal law to facilitate urgently needed research regarding the efficacy of cannabis and related cannabinoids. Federal regulations impede the necessary research to determine the therapeutic benefits of cannabis and related cannabinoids for disease-related symptoms and side effects. The ANA position statement does not extend to the current debate about legalizing cannabis for recreational purposes (ANA, 2021). In their position statement, the ANA emphasizes support for the following:
- “Scientific review of cannabis’s status as a federal Schedule I controlled substance and relisting cannabis as a federal Schedule II controlled substance for purposes of facilitating research;
- Development of prescribing standards that include indications for use, specific dose, route, the expected effect, and possible side effects, as well as indications for stopping a medication;
- Establishing evidence-based standards for the use of cannabis and related cannabinoids;
- Protection from criminal or civil penalties for patients using therapeutic cannabis and related cannabinoids as permitted under state laws;
- Exemption from criminal prosecution, civil liability, or professional sanctioning, such as loss of licensure or credentialing, for health care practitioners who discuss treatment alternatives concerning cannabis or who prescribe, dispense, or administer cannabis in accordance with professional standards and state laws.” (ANA, 2021, pp. 1–2).
Future Research
Regarding the future of cannabis and cannabinoid use in health care, many researchers feel that the future of cannabis in health care is not likely with cannabis as a whole but instead in distilling and purifying the most therapeutic components to ensure a reliable, pure, and consistent product that can stand up to the strict standards put forth by the FDA. This may include products containing CBD that may function as antipsychotics, antiseizure, or treatments for addiction. Other suggestions for future research include a CB1 antagonist for elevated body mass index (BMI) or addiction treatment, a synthetic CB2 agonist as an anti-inflammatory in the treatment of scleroderma, or a mixture of cannabinoids for the treatment of diabetes or metabolic syndrome. Long-term studies are needed to evaluate the clinical efficacy for chronic conditions such as chronic pain, epilepsy, MS, and other neurodegenerative diseases, such as Alzheimer’s. In addition to long-term studies, future research should also explore the efficacy of cannabis for specific populations, including pregnant individuals, older adults, and adolescents (Hossain & Chae, 2024). The National Institute on Drug Abuse (NIDA) funds research on the endocannabinoid system, cannabinoid compounds, and health effects of cannabis. In addition, they support policy, public health, and epidemiology research related to cannabis use. The NIDA also funds research on the potential therapeutic effects of cannabis and cannabinoids to reduce the use of other substances such as opioids. They also focus on the safety of cannabis use, including the development of new treatments for cannabis use disorder (NIDA, 2024).
References
AlHabil, Y., Saadeddin, L., Ishkirat, H., Alqam, M., Hossoon, O., Hameedi, S., Yacoub, H., Yasin, D., Bahbah, A., Oweidat, M., & Mosa, H. (2026). Assessing the role of cannabis in managing spasticity in multiple sclerosis: A systematic review and meta-analysis. Clinical Therapeutics, 48(1), 13–21. https://doi.org/10.1016/j.clinthera.2025.07.009
Allan, G. M., Finley, C. R., Ton, J., Perry, D., Ramji, D., Crawford, K., Lindblad, A. J., Korownyk, C., & Kolber, M. R. (2018). Systematic review of systematic reviews for medical cannabinoids: Pain, nausea and vomiting, spasticity, and harms. Canadian Family Physician, 64(2), e78–e94. https://pmc.ncbi.nlm.nih.gov/articles/PMC5964405
American Cancer Society. (2025). Cannabis and cancer. https://www.cancer.org/cancer/supportive-care/integrative-medicine/cannabis.html
American Nurses Association. (2021). Therapeutic use of marijuana and related cannabinoids. https://www.nursingworld.org/globalassets/practiceandpolicy/nursing-excellence/ana-position-statements/therapeutic-use-of-marijuana-and-related-cannabinoids-position-statement-final-2021.pdf
Bach, C. (2025). About: Megestrol (Megace®, Megace-ES®). OncoLink. https://www.oncolink.org/cancer-treatment/oncolink-rx/megestrol-megace-r-megace-es-r
Bell, A. D., MacCallum, C., Margolese, S., Walsh, Z., Wright, P., Daeninck, P. J., Mandarino, E., Lacasse, G., Deol, J. K., de Freitas, L., St Pierre, M., Belle-Isle, L., Gagnon, M., Bevan, S., Sanchez, T., Arlt, S., Monahan-Ellison, M., O’Hara, J. O., Boivin, M., & Costiniuk. C. (2024). Clinical practice guidelines for cannabis and cannabinoid-based medicines in the management of chronic pain and co-occurring conditions. Cannabis and Cannabinoid Research, 9(2), 669–687. https://doi.org/10.1089/can.2021.0156
Bilbao, A., & Spanagel, R. (2022). Medical cannabinoids: A pharmacology-based systematic review and meta-analysis for all relevant medical indications. BMC Medicine, 20(1), 259. https://doi.org/10.1186%2Fs12916-022-02459-1
Bridgeman, M. B., & Abazia, D. T. (2017). Medicinal cannabis: History, pharmacology, and implications for the acute care setting. Pharmacy and Therapeutics, 42(3), 180–188. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5312634
Buppert, C., & Klein, T. A. (2021). Certifying medical cannabis: What APRNs need to know. Medscape. https://www.medscape.com/viewarticle/943249
Centers for Disease Control and Prevention. (2024). State medical cannabis laws. https://www.cdc.gov/cannabis/about/state-medical-cannabis-laws.html
Cheng, K. Y. C., Harnett, J. E., Davis, S. R., Eassey, D., Law, S., & Smith, L. (2022). Healthcare professionals’ perspectives on the use of medicinal cannabis to manage chronic pain: A systematic search and narrative review. Pain Practice, 22(8), 718–732. https://doi.org/10.1111/papr.13161
Filippini, G., Minozzi, S., Borrelli, F., Cinquini, M., & Dwan, K. (2022). Cannabis and cannabinoids for symptomatic treatment for people with multiple sclerosis. Cochrane Database of Systematic Reviews, (5), CD013444. https://doi.org/10.1002/14651858.CD013444.pub2
Fischer, B., Robinson, T., Bullen, C., Curran, V., Jutras-Aswad, D., Medina-Mora, M. E., Pacula, R. L., Rehm, J., Room, R., van den Brink, W., & Hall, W. (2022). Lower-risk cannabis use guidelines (LRCUG) for reducing health harms from non-medical cannabis use: A comprehensive evidence and recommendations update. International Journal of Drug Policy, 99, 103381. https://doi.org/10.1016/j.drugpo.2021.103381
Haddad, F., Dokmak, G., & Karaman, R. (2022). The efficacy of cannabis on multiple sclerosis-related symptoms. Life, 12(5), 682. https://doi.org/10.3390/life12050682
Haney, B. (2023). 35th annual APRN legislative update: Updates to APRN practice authority in the United States. The Nurse Practitioner, 48(1), 20–47. https://doi.org/10.1097/01.NPR.0000903012.03553.a4
Hesketh, P. J. (2024). Management of poorly controlled or breakthrough chemotherapy-induced nausea and vomiting in adults. UpToDate. Retrieved April 11, 2026, from https://www.uptodate.com/contents/management-of-poorly-controlled-or-breakthrough-chemotherapy-induced-nausea-and-vomiting-in-adults
Hossain, M. K., & Chae, H. J. (2024). Medical cannabis: From research breakthroughs to shifting public perceptions and ensuring safe use. Integrative Medicine Research, 13(4), 101094. https://doi.org/10.1016/j.imr.2024.101094
Martinez Naya, N., Kelly, J., Corna, G., Golino, M., Abbate, A., & Toldo, S. (2023). Molecular and cellular mechanisms of action of cannabidiol. Molecules, 28(16), 5980. https://doi.org/10.3390/molecules28165980
Mouhamed, Y., Vishnyakov, A., Qorri, B., Sambi, M., Frank, S. M. S., Nowierski, C., Lamba, A., Bhatti, U., & Szewczuk, M. R. (2018). Therapeutic potential of medicinal marijuana: An educational primer for health care professionals. Drug, Healthcare, and Patient Safety, 10, 45–66. https://doi.org/10.2147/dhps.s158592
Mücke, M., Phillips, T., Radbruch, L., Petzke, F., & Häuser, W. (2018). Cannabis-based medicines for chronic neuropathic pain in adults. Cochrane Database of Systematic Reviews (3), CD012182. https://doi.org/10.1002/14651858.CD012182.pub2
National Cancer Institute. (2025). Cannabis and cannabinoids (PDQ®)—Health professional version. https://www.cancer.gov/about-cancer/treatment/cam/hp/cannabis-pdq#_13
National Conference of State Legislatures. (2025). State medical cannabis laws. https://www.ncsl.org/health/state-medical-cannabis-laws
National Institute on Drug Abuse. (2024). Cannabis (marijuana). https://nida.nih.gov/research-topics/cannabis-marijuana#NIDA-researching-cannabis
Neuhofer, Z. T., Sacco, L. N., & Sheikh, H. Z. (2025). Change to federal definition of hemp and implications for federal enforcement. https://www.congress.gov/crs-product/IN12620
Office of Cannabis Management. (n.d.). Medical cannabis program FAQs. Retrieved April 12, 2026, from https://cannabis.ny.gov/medical-cannabis-program-faqs
Patel, P., Turner, A. R., & Agrawal, S. (2024). Cannabis (marijuana) overview. In StatPearls [Internet]. https://www.ncbi.nlm.nih.gov/books/NBK430801
Pew Research Center. (2024). Most Americans favor legalizing marijuana for medical, recreational use. https://www.pewresearch.org/politics/2024/03/26/most-americans-favor-legalizing-marijuana-for-medical-recreational-use
Razmovski-Naumovski, V., Luckett, T., Amgarth-Duff, I., & Agar, M. R. (2022). Efficacy of medicinal cannabis for appetite-related symptoms in people with cancer: A systematic review. Palliative Medicine, 36(6), 912–927. https://doi.org/10.1177/02692163221083437
Schachter, S. C., & Sirven, J. I. (2026). Antiseizure medications: Mechanism of action, pharmacology, and adverse effects. UpToDate. Retrieved April 10, 2026, from https://www.uptodate.com/contents/antiseizure-medications-mechanism-of-action-pharmacology-and-adverse-effects
Shane-McWhorter, L. (2025). Cannabidiol (CBD). https://www.merckmanuals.com/professional/special-subjects/dietary-supplements/cannabidiol-cbd
Sheikh, H. S. (2026). The federal status of marijuana and the policy gap with states. Congressional Research Service. https://www.congress.gov/crs_external_products/IF/PDF/IF12270/IF12270.9.pdf
Slawek, D., & Arnsten, J. H. (2025). Medical use of cannabis and cannabinoids in adults. UpToDate. Retrieved April 8, 2026, from https://www.uptodate.com/contents/medical-use-of-cannabis-and-cannabinoids-in-adults
Stanciu, C. N., Brunette, M. F., Teja, N., & Budney, A. J. (2021). Evidence for use of cannabinoids in mood disorders, anxiety disorders, and PTSD: A systematic review. Psychiatric Services, 72(4), 429–436. https://doi.org/10.1176/appi.ps.202000189
Szaflarski, J. P., Bebin, E. M., Comi, A. M., Patel, A. D., Joshi, C., Checketts, D., Beal, J. C., Laux, L. C., DeBoer, L. M., Wong, M. H., Lopez, M., Devinsky, O., Lyons, P. D., Zentil, P. P., Wechsler, R., & CBD EAP study group. (2018). Long-term safety and treatment effects of cannabidiol in children and adults with treatment-resistant epilepsies: Expanded access program results. Epilepsia, 59(8), 1540–1548. https://doi.org/10.1111/epi.14477
Szaflarski, J. P., Bebin, E. M., Cutter, G., DeWolfe, J., Dure, L. S., Gaston, T. E., Kankirawatana, P., Liu, Y., Singh, R., Standaert, D. G., Thomas, A. E., Ver Hoef, L. W., & UAB CBD program. (2018). Cannabidiol improves frequency and severity of seizures and reduces adverse events in an open-label add-on prospective study. Epilepsy & Behavior, 87, 131–136. https://doi.org/10.1016/j.yebeh.2018.07.020
Tomko, A. M., Whynot, E. G., Ellis, L. D., & Dupré, D. J. (2020). Anti-cancer potential of cannabinoids, terpenes, and flavonoids present in cannabis. Cancers, 12(7), 1985. https://doi.org/10.3390/cancers12071985
US Department of Health and Human Services. (2015). Announcement of revision to the Department of Health and Human Services guidance on procedures for the provision of marijuana for medical research as published on May 21, 1999. https://www.federalregister.gov/documents/2015/06/23/2015-15479/announcement-of-revision-to-the-department-of-health-and-human-services-guidance-on-procedures-for
US Department of Justice. (2024). Justice Department submits proposed regulation to reschedule marijuana. https://www.justice.gov/archives/opa/pr/justice-department-submits-proposed-regulation-reschedule-marijuana
US Food and Drug Administration. (2023). FDA and cannabis: Research and drug approval process. https://www.fda.gov/news-events/public-health-focus/fda-and-cannabis-research-and-drug-approval-process
US Food and Drug Administration. (2024). FDA regulation of cannabis and cannabis-derived products, including cannabidiol (CBD). https://www.fda.gov/news-events/public-health-focus/fda-regulation-cannabis-and-cannabis-derived-products-including-cannabidiol-cbd#farmbill
The White House. (2025). Increasing medical marijuana and cannabidiol research. https://www.whitehouse.gov/presidential-actions/2025/12/increasing-medical-marijuana-and-cannabidiol-research
Zammit Dimech, D., Grech, L., & Serracino Inglott, A. (2025). Doctors’ and pharmacists’ perspectives on the clinical use of medicinal Cannabis: A cross-sectional study. Harm Reduction Journal, 22, 167. https://doi.org/10.1186/s12954-025-01317-6
Powered by Froala Editor