About this course:
This course will provide an overview of the pathophysiology of pain, the components of a comprehensive pain assessment, and discuss nonpharmacological and nonopioid pharmacological management of pain. It will also discuss the core aspects of prescribing opioids for pain, including best-practice opioid prescribing guidelines, proper monitoring of patients on long-term opioid therapy, and the clinical features of opioid misuse/opioid use disorder (OUD).
Course preview
Pain Management for APRNs
Pain Management APRN Disclosure.docx
This course will provide an overview of the pathophysiology of pain, the components of a comprehensive pain assessment, and discuss nonpharmacological and nonopioid pharmacological management of pain. It will also discuss the core aspects of prescribing opioids for pain, including best-practice opioid prescribing guidelines, proper monitoring of patients on long-term opioid therapy, and the clinical features of opioid misuse/opioid use disorder (OUD).
Upon completion of this module, learners should be able to:
- define pain, discuss the pathophysiology of pain, and recognize the four main categories of pain
- identify the core components of a comprehensive pain assessment and describe the use of pain assessment scales and tools
- review the different types of nonpharmacological pain management strategies and interventional pain management procedures
- discuss the pharmacological management of pain using nonopioid and adjuvant analgesics
- define opioids and distinguish between opioid agonists, partial agonists, mixed agonist-antagonists, and opioid antagonists, and identify specific medications within each category
- demonstrate competency in best-practice opioid prescribing guidelines, including the proper prescribing and monitoring of patients on long-term opioid therapy
- discuss how to taper long-term opioid use and appropriate steps to take when terminating chronic opioid therapy
- recognize the potential for opioid misuse and abuse, the key features of OUD, and strategies to mitigate opioid misuse and OUD
Pain is a subjective individual experience for each person. In 1968, Margo McCaffery, a pioneer and world-renowned expert in pain management, defined pain as "… whatever the experiencing person says it is, existing whenever he says it does" (McCaffery, 1968). In 2020, the International Association for the Study of Pain (IASP) revised its definition of pain for the first time since 1979 to the following: "an unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage" (IASP, 2021). Pain cannot be objectively measured and depends on the individual's self-report. It is a complex perception with physiological, behavioral, and psychological components, with wide variability in each person's experience. Nevertheless, pain is a common reason individuals seek medical care. Advanced practice registered nurses (APRNs) must understand pain's underlying mechanisms and clinical features to develop safe, effective, and personalized treatment plans (National Institute of Neurological Disorders and Stroke [NINDS], 2026a; Tauben & Stacey, 2026b; Wager, 2022).
Pathophysiology of Pain
The purpose of pain is to prevent tissue damage and protect the body while healing, although its etiology is complex and multifaceted. The mechanism by which a stimulus is perceived as painful by the brain is not fully understood. Pain can be caused by mechanical, chemical, or thermal means. Mechanical pain is induced by trauma, injury, or overuse. It may be constant, variable, or intermittent. Chemical pain is associated with inflammatory disorders, and thermal pain is due to excessive heat or cold exposure. Neurons are messengers in the body responsible for connecting, receiving, and processing pain. They use electrical and chemical signals to transfer information between the brain, the spinal cord, and the rest of the body. Fundamentally, pain is felt when sensory nerve endings called nociceptors (or pain receptors) come in contact with a noxious (painful) stimulus. The noxious stimulus triggers three chief events: transduction, transmission, and modulation (refer to Table 1). A nerve impulse travels from the sensory nerve ending to the spinal cord, rapidly propelling it to the brain via the spinal cord and brainstem. The brain processes the painful sensation and responds with a motor response to terminate the inciting event. There are three primary types of neurons. Primary sensory neurons in the peripheral nervous system conduct painful sensations from the periphery to the dorsal root of the spinal cord. Secondary sensory neurons in the spinal cord or brainstem transmit the painful sensation to the thalamus. Tertiary sensory neurons communicate the painful sensation from the thalamus to the somatosensory areas of the cerebral cortex. Table 1 defines the primary pain processes and reviews important terminology (Barad & Aggarwal, 2026; Cao et al., 2024; NINDS, 2026a; Wager, 2022).
Table 1
Pain Processes: Terms and Definitions
Transduction is the conversion of noxious stimuli to an electrical impulse through specialized peripheral nerve fibers, also called nociceptors. Nociceptors are found throughout the body and activate a series of events in response to painful stimuli. The nerve endings detect mechanical, thermal, or chemical stimuli. Transduction occurs before the next process, transmission. |
Transmission occurs as the electrical impulse travels along the nerve fibers, where neurotransmitters regulate it. The signal is then transmitted to the dorsal horn of the spinal cord, where it is either dampened or amplified before being sent to the brain.
|
Modulation is the final process in the spinal cord; it causes muscles to contract reflexively, moving the body away from the painful stimuli. |
Perception occurs across various areas of the brain, influenced by thought and emotional processes. It refers to the patient's conscious awareness of pain as a culmination of pathophysiological processes and prior experiences. |
|
olid; border-color: currentcolor windowtext windowtext; border-image: initial; padding: 0in 5.4pt;"> The pain threshold is the point at which a person feels pain. |
A person's pain tolerance is the maximum intensity of a pain-producing stimulus they are willing to accept in each situation. |
Neurotransmitters are chemicals released by neurons throughout the nervous system in response to cellular damage. They bind to and activate protein receptors on the surface of cells, which function as a gate to inhibit (block) or excite (transmit) a signal. Some of the neurotransmitters involved in the pain process include the following:
|
(Barad & Aggarwal, 2026; Cao et al., 2024; Ignatavicius et al., 2024; NINDS, 2026a)
The two major classes of nerve fibers associated with pain transmission include unmyelinated C fibers and myelinated A-delta fibers. Unmyelinated C fibers conduct impulses slowly and respond to thermal, mechanical, and chemical stimuli. They generate dull, aching, burning, diffuse, and delayed pain sensations. Myelinated A-delta fibers conduct impulses more rapidly, respond to mechanical (pressure) stimuli, and generate sharp, localized, and fast pain sensations. The spinothalamic tract is one of the central pain pathways. It originates in the spinal cord and extends to the thalamus. It transmits sensory information regarding pain, temperature, and touch. The spinoreticular tract is excited by similar sensory fibers as the spinothalamic tract, but instead of ascending to the thalamus, it terminates in the brainstem. Typically, there are two routes for conducting signal transmissions: ascending and descending. The ascending pathway travels upward, carrying sensory information from the body via the spinal cord toward the brain. The descending path travels downward from the brain to the organs via the spinal cord (Cao et al., 2024; NINDS, 2026a).
Categories of Pain
Pain is primarily categorized by duration (acute [less than 1 month], subacute [1–3 months], and chronic [greater than 3 months]). It is also classified by origin (nociceptive, neuropathic, or nociplastic) or the disease or condition that causes it (e.g., cancer, diabetes, rheumatoid arthritis [RA], etc.). Nociceptive pain includes somatic pain (skin, muscles, and soft tissues) and visceral pain (internal organs and lining of body cavities; Dowell et al., 2022; IASP, 2021; Ignatavicius et al., 2024; NINDS, 2026a).
Acute Pain
Acute pain is a warning sign or protective response that something in the body has been damaged, notifying the individual to respond to or escape the painful stimuli. It usually has a direct cause, resulting from disease, inflammation, or tissue injury. The etiology of acute pain is infinite, such as surgery, burns, invasive procedures, childbirth, or trauma. It is temporary and self-limiting, meaning it is confined to a defined period and often resolves with tissue healing. Acute pain may be accompanied by anxiety or emotional distress. Physiological responses to acute pain include activating the sympathetic nervous system or the body's inherent fight-or-flight response. Manifestations of the sympathetic response may include tachycardia, hypertension, increased respiratory rate, dilated pupils, diaphoresis, anxiety, and muscle tension. Behavioral responses to acute pain may consist of restlessness, moaning, flinching, grimacing, guarding, apprehension, and an inability to concentrate. Acute pain is usually treatable, and interventions aim to address the underlying cause. However, if left untreated or unrelieved, acute pain can become maladaptive and lead to chronic pain (Ignatavicius et al., 2024; NINDS, 2026a).
Subacute Pain
Subacute pain is a subset of acute pain, where the duration of pain falls between acute and chronic pain. It is a relatively new concept recently incorporated into the updated Centers for Disease Control and Prevention (CDC) guidance on pain management. Subacute pain lasts 4–12 weeks, with common causes presenting as low back pain, neck pain, and muscle strains (CDC, 2024a; Chou, 2026).
Chronic Pain
Chronic pain is a widely prevalent condition and is one of the most common reasons people seek health care services. According to the 2023 National Health Interview Survey, an estimated 24.3% of the adult population had chronic pain, and 8.5% experienced high-impact chronic pain (i.e., chronic pain that results in a substantial restriction to daily activities). This is an overall increase from 2021, when an estimated 20.4% of the adult population had chronic pain, and 7.4% experienced high-impact chronic pain. American Indian and Alaska Native non-Hispanic adults reported more chronic pain (30.7%) than Asian non-Hispanic adults (11.8%) and Hispanic adults (17.1%). Female patients also reported more chronic pain and high-impact chronic pain than men. The prevalence of chronic pain and high-impact chronic pain also increased with age (Lucas & Sohi, 2024). Chronic pain does not serve as a protective function and is instead a pathologic (or dysfunctional) process. The onset is typically gradual, and symptoms are ongoing, unrelenting, persisting beyond tissue healing, and lasting longer than 3 months. Chronic pain is often poorly localized and can be challenging to describe. Although chronic pain does not have the physiological response on the sympathetic nervous system that acute pain does, it is associated with significant morbidity, including disparaging physical and mental health conditions. In the United States, chronic pain has been linked with depression, Alzheimer's disease (and related dementias), higher suicide risk, and substance use disorders (SUDs). Patients with chronic pain are also at higher risk for fatigue, functional impairment, disability, and financial burden. Chronic pain can interfere with personal and intimate relationships and contribute to social isolation or emotional distress. Management is aimed at symptomatic relief, although it is more resistant to medical treatment than acute pain and does not always respond to conventional interventions. If the underlying etiology cannot be identified, controlling the long-term effects of the pain is particularly challenging. Chronic pain can be idiopathic, meaning it has no identifiable cause (Barad & Aggarwal, 2026; Ignatavicius et al., 2024; Taylor et al., 2022).
One of the most common conditions causing chronic pain is low back pain. It is one of the leading causes of disability in Americans, as an estimated 84% of adults are affected at some point in their lives. Low back pain profoundly affects patients, families, work productivity, and the economy. Determining the cause of low back pain can be difficult and expensive. Low back pain can result from a prior injury that did not resolve or heal properly, poor body mechanics and posture, or wear-and-tear associated with aging (e.g., osteoarthritis [OA] and degenerative disc disease). Cancer-related pain is often considered a chronic pain condition attributed to tumor invasion, nerve compression, bone metastases, or as a byproduct of treatment, such as radiation therapy (Ignatavicius et al., 2024; Taylor et al., 2022; Wheeler et al., 2026).
Fibromyalgia is another common cause of chronic pain. It is a poorly understood chronic pain condition characterized by abnormal pain perception processing that affects about 2%–5% of people. The etiology is unknown, but it is typically classified as a nociplastic or central sensitization form of pain. Patients experience a range of symptoms, including diffuse musculoskeletal pain, stiffness, fatigue, exercise intolerance, headaches, sleep disturbance, and cognitive impairment (e.g., memory and concentration problems). Fibromyalgia more commonly affects middle-aged females and patients with RA or lupus (Goldenberg & Kaplan, 2025a). The condition is treated with a combination of pharmacological and nonpharmacological interventions. Recommended lifestyle modifications include aerobic exercise, stress management, cognitive-behavioral therapy, and sleep hygiene (Goldenberg & Kaplan, 2025b). Table 2 provides a comparison chart of acute and chronic pain features.
Table 2
Acute Versus Chronic Pain
Acute Pain | Chronic Pain |
Short duration, temporary, reversible | Longer duration (usually lasts more than 3 months), ongoing, long-lasting, and may be irreversible |
Localized and generally has a well-defined etiology | Often poorly localized and may not have a well-defined etiology |
Pain is acute and declines with tissue healing | Pain is gradual and persists, even without an identifiable injury or cause |
May ignite the sympathetic nervous system's “fight or flight” response | Does not impact the sympathetic nervous system function |
(Arcangelo et al., 2022; Ignatavicius et al., 2024; Taylor et al., 2022)
Nociceptive Pain
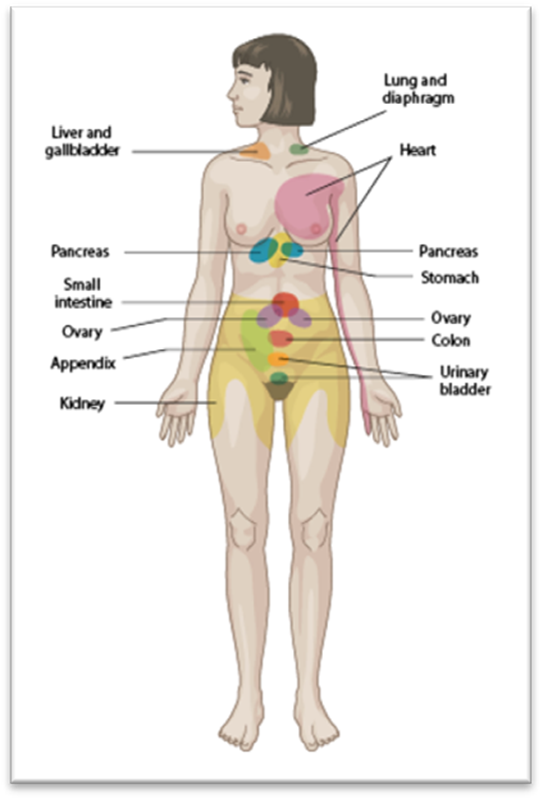
Nociceptive pain is the physiologic response arising from tissue injury or damage caused by a noxious stimulus. There are two main categories of nociceptive pain: somatic and visceral. Somatic pain is further subdivided by the location of the pain receptors, which includes cutaneous or superficial (skin and subcutaneous tissues) and deep somatic (fascia, musculoskeletal, blood vessels, bone, joint capsules, and connective tissues). Stimulation of somatic pain receptors typically produces well-localized pain that may be described as sharp, dull, aching, or burning. Examples of somatic pain include incisional pain, wound complications, muscle spasms, and peripheral vascular disease. Visceral pain receptors are located within internal organs, the lining of the body cavities (e.g., stomach or intestines), and surrounding connective tissue. Visceral pain is poorly localized, diffuse, and described as deep cramping, sharp, or shooting. Examples of visceral pain include colitis, pancreatitis, bladder spasms, and appendicitis. Visceral pain from an injury to an organ capsule or other deep connective tissues may also be described as sharper and more localized. As shown in Figure 1, visceral pain can cause referred pain in different body locations separate from the site of the noxious stimulus (Barad & Aggarwal, 2026; Ignatavicius et al., 2024; Tauben & Stacey, 2026a).
Figure 1
Map of Referred Visceral Pain
Neuropathic Pain
Neuropathic pain results from damage to or dysfunction of the nervous system, inducing hyperalgesia (i.e., pain out of proportion to the injury). Neuropathic pain is usually described as intense, shooting, or burning and can be characterized by sensory abnormalities, such as paresthesia (e.g., numbness, tingling, or "pins and needles"). Allodynia, or pain due to a stimulus that does not normally provoke pain, is another common manifestation of neuropathic pain. The pain may occur in an area other than the one stimulated. Opioid use in patients with neuropathic pain is controversial, as opioids are not typically effective. First-line pharmacologic therapy typically includes antiseizure medications, antidepressants, and antispasmodics. Many types of neuropathic pain conditions are chronic and relentless. Four common neuropathic pain conditions are described below: postherpetic neuralgia (PHN), trigeminal neuralgia, diabetic neuropathy, and phantom limb pain (Ignatavicius et al., 2024; Tauben & Stacey, 2026a).
Postherpetic Neuralgia
PHN is a highly painful and debilitating complication of the herpes zoster (Shingles) virus. Shingles is caused by the reactivation of the varicella-zoster virus (VZV), which lies dormant in the dorsal root ganglia of the spinal cord following varicella (chickenpox) infection. While a typical shingles rash resolves within a few weeks, PHN results from damage to sensory nerves, affecting nerve fibers and the skin, and can persist for weeks, months, or longer. Diagnosis is made when the pain occurs or persists for 90 days or more after the onset of shingles. An estimated 5%–20% of people who develop shingles will have PHN. The risk for PHN is more likely in older adults, females, White individuals, and people who are immunocompromised. Hyperalgesia and allodynia following the resolution of the skin rash are among PHN's most prominent clinical manifestations. Antiviral medicines are recommended for treating shingles, as they decrease the length and severity of the illness. Antivirals are most effective when initiated immediately (ideally within 48 hours) after the first symptoms appear; however, it is unclear whether antiviral treatment reduces the risk of PHN (Ignatavicius et al., 2024; Kissoon, 2026). The recommended antiviral treatment options for immunocompetent adolescents and adults with shingles include one of the following:
- valacyclovir (Valtrex) 1 g twice daily
- famciclovir (Famvir) 250 mg three times daily or 500 mg twice daily
- acyclovir (Zovirax) 400 mg orally three times daily or 200 mg five times daily (Wald & Johnston, 2024)
Treatment of PHN is challenging, and effective relief often requires a multidisciplinary approach. Adjunctive topical and nonpharmacologic strategies to reduce pain include topical lidocaine (Lidoderm) patches, topical capsaicin (Salonpas), behavioral therapy (mindfulness and cognitive behavioral therapy), and acupuncture. Commonly prescribed pharmacologic agents include the following:
- tricyclic antidepressants (TCAs) such as nortriptyline (Pamelor) and amitriptyline (Elavil)
- serotonin-norepinephrine reuptake inhibitors (SNRIs) such as duloxetine (Cymbalta) and venlafaxine (Effexor)
- gabapentinoids such as gabapentin (Neurontin) and pregabalin (Lyrica; Kissoon, 2026)
To prevent this debilitating condition and its associated complications, the shingles vaccination is recommended for all adults aged 50 and older (immunocompromised and immunocompetent). The CDC recommends the recombinant zoster vaccine (RZV, Shingrix) be administered as a two-dose series, two to 6 months apart. It is also recommended for adults aged 19 and older who are immunocompromised from any condition or therapy (CDC, 2025a; Wald & Johnston, 2024).
Trigeminal Neuralgia (TN)
TN, or tic douloureux, is a severe pain condition affecting the fifth cranial nerve, inducing excruciating, shock-like burning pain. It usually affects one side of the face near the jaw or cheek, and the intensity of the pain is so severe that it can be physically and mentally debilitating. TN pain can be sporadic and intermittent, often called "attacks of pain,” that occur regularly for days to weeks or longer. Pain attacks occur several times daily and can be triggered by contact with the face or cheek (such as brushing teeth, applying makeup, eating, or light touch). Diagnosis and treatment of the condition are equally complex. Management involves a combination of pharmacological and nonpharmacological strategies. Most patients do not find relief from traditional pain-relieving medications such as acetaminophen (Tylenol), nonsteroidal anti-inflammatory drugs (NSAIDs), or opioids. Carbamazepine (Tegretol) or oxcarbazepine (Trileptal) is recommended as initial medical management of TN. Other pharmacologic therapies include gabapentin (Neurontin), lamotrigine (Lamictal), or baclofen (Lioresal). Common nonpharmacological therapies used alongside medications for TN include acupuncture, biofeedback, aromatherapy, meditation, and vitamin therapy. Surgical treatment may be advised if all other management strategies fail (Ho et al., 2026; NINDS, 2026b).
Diabetic Neuropathy
Diabetic neuropathy is nerve damage caused by diabetes or poor blood glucose control over time. It can develop slowly after many years of elevated blood glucose levels or occur relatively early in the disease. There are a few types of diabetic neuropathies depending on which nerves are damaged, but the most common is peripheral neuropathy, which affects the legs, feet, and toes. Diabetes is the most common cause of peripheral neuropathy, and painful diabetic neuropathy occurs in an estimated 30% of patients with diabetes (Feldman, 2025). Diabetic neuropathy can impair movement and cause problems with balance and coordination. It can also affect how people process sensations (e.g., hot and cold), leading to muscle weakness and other complications such as foot infections and ulcers. People with diabetes may also experience focal neuropathies, such as damage to a single nerve in a specific body part, called entrapment syndromes. Autonomic neuropathy also occurs in people with diabetes, which damages the nerves that control the internal organs. Autonomic neuropathy can lead to digestive dysfunction, bladder dysfunction, or ocular retinopathy. These conditions can contribute to the overall morbidity among this population. Nonpharmacologic treatment strategies include proper foot hygiene, wearing appropriate footwear, weight loss, and physical therapy (PT, including balance and gait training; Feldman, 2025).
The American Academy of Neurology (AAN; Price et al.) 2021 practice guideline update on the treatment of painful diabetic neuropathy supports the following treatment options for diabetic neuropathy:
- TCAs, such as nortriptyline (Pamelor), amitriptyline (Elavil), and imipramine (Tofranil)
- gabapentinoids such as gabapentin (Neurontin) and pregabalin (Lyrica)
- SNRIs, such as duloxetine (Cymbalta), venlafaxine (Effexor), and desvenlafaxine (Pristiq)
- antiseizure medications such as oxcarbazepine (Trileptal), lamotrigine (Lamictal), and valproic acid (Depakene)
- SNRI/opioid dual mechanism agents such as tramadol (Ultram) and tapentadol (Nucynta; Price et al., 2021)
Although some of these medications are not approved by the US Food and Drug Administration (FDA) specifically to treat diabetic neuropathy, duloxetine (Cymbalta), pregabalin (Lyrica), tapentadol ER (Nucynta), and capsaicin 8% topical system (Qutenza) are all FDA-approved for this indication. The FDA has also approved spinal cord stimulation devices for the treatment of refractory, painful diabetic neuropathy (Mallick-Searle & Adler, 2024).
Phantom Limb Pain
Phantom limb pain is the perception of pain in a limb that no longer exists. This is diagnosed after all other potential causes have been excluded, such as ischemia, neuroma, infection, and pressure wounds. The incidence ranges from 52% to 88% (Kalapatapu, 2025). After losing a body part, affected individuals describe phantom limb pain as stabbing, shooting, burning, and throbbing. Allodynia is a common manifestation. Risk factors include older age at the time of amputation, lower limb amputation, and bilateral limb amputation. Treatment is complex and often requires a combination of strategies. Nonpharmacologic therapies include mirror therapy, virtual reality, peripheral nerve stimulation, heat application, PT, biofeedback, transcutaneous electrical nerve stimulation (TENS), massage, and acupuncture. Pharmacologic treatments include injections with local anesthetics and/or steroids, nerve blocks, NSAIDs, opioids, antidepressants, antiseizure medications, and muscle relaxants (Ignatavicius et al., 2024; Kalapatapu, 2025).
Nociplastic Pain
When the pain is not caused by clear tissue injury or nerve damage, it is termed nociplastic. There is no evidence of a disease process, lesion, or tissue damage to explain the pain. While this term may not be encountered in the clinical setting, it was designed to better understand chronic pain conditions. This type of pain may augment other types and be accompanied by hypersensitivity to odors, light, and sound. Four nociplastic pain condition examples include fibromyalgia, irritable bowel syndrome, chronic pelvic pain, and interstitial cystitis (IASP, 2021; Tauben & Stacey, 2026b).
Risk Factors for Pain
Several risk factors have been reported to increase the risk of pain. Some of the most common include the following:
- genetics
- advancing age and frailty
- lower socioeconomic status
- occupational-associated risks (e.g., manual labor involving heavy lifting or inactivity due to a desk job, poor posture, and improper body mechanics)
- low health literacy
- preexisting mental health conditions
- sedentary lifestyle, being overweight or obese
- SUDs
- presence of specific underlying health conditions such as cancer, sickle cell disease, autoimmune disorders, arthritis, fibromyalgia, and neuropathy
- trauma or surgery(s)
- invasive diagnostic or treatment procedures (NINDS, 2026a; Tauben & Stacy, 2026b)
Factors Affecting the Pain Experience
APRNs must be cognizant of the numerous factors that affect a patient's pain experience, which can complicate the diagnostic workup. Some of the most common factors that impact the individual pain experience are listed in Table 3.
Table 3
Factors Impacting the Pain Experience
Age | Age can influence how pain is perceived, diagnosed, and treated.
|
Cognitive function | Patients who are cognitively impaired may be unable to report pain or describe it accurately. |
Fatigue | Fatigue can heighten pain sensitivity. |
Genetic sensitivity | Genetics can increase or decrease pain tolerance. |
Prior experience | Prior experiences with pain can increase or decrease sensitivity, depending on whether adequate pain relief was obtained. |
Anxiety | Anxiety and fear can increase pain sensitivity. |
Support and coping | Support systems and coping styles can impact the pain experience positively or negatively. For example, positive coping skills and robust social support systems can decrease sensitivity to pain, whereas poor coping skills or a lack of support can heighten pain sensitivity. |
Culture | Culture influences how patients may express pain or the meaning they attach to pain. For example, some cultures consider pain as a sign of weakness and discourage people from openly reporting or describing pain. |
(Berger & O’Neill, 2022; US Department of Health and Human Services [HHS], 2019)
Risk Factors for the Undertreatment of Pain
The undertreatment of pain is a severe problem across the United States that has been intensified by the opioid epidemic and restrictions on opioid prescribing guidelines in recent years. While certain laws, regulations, and policies that seemed to align with the 2016 CDC Opioid Prescribing Guideline may have benefited some individuals, the guidelines were intended to be adaptable to support individual patients. A significant concern is that some of these policies diverged from their intent, and misapplication contributed to untreated and undertreated pain. Examples included imposing duration limits by insurers and pharmacies, rigid dosage thresholds, and dismissing or abandoning patients. Additionally, the ongoing issue of untreated or inadequately treated pain due to biases continues to require urgent and sustained attention and action. In 2022, the CDC released a new clinical practice guideline for prescribing opioids for pain, which replaced those from 2016. This guideline will be discussed later in this course (Dowell et al., 2022).
Undertreated pain severely impacts physical and mental health, such as increased anxiety with acute pain and depression with chronic pain. According to the US Department of Health and Human Services (HHS, 2019), some of the most common risk factors associated with the undertreatment of pain include:
- cultural and societal attitudes toward pain (stigma)
- lack of knowledge and education regarding pain and appropriate management
- fear of addiction among patients and healthcare providers (HCPs)
- reduced HCP willingness to prescribe opioids due to legislative changes and perceived liability and legal consequences
- the exaggerated fear of respiratory depression
- barriers to accessing care (lack of insurance coverage and payment for pain modalities or access to pain specialists)
- specific populations: infants and children, older adults, and patients with SUD (HHS, 2019)
Pain Assessment
All patients should be screened for pain as the first step in a comprehensive pain assessment. The most valid pain assessment is self-report, although this can be influenced by several factors (e.g., mood, culture, cognitive abilities, etc.). Since pain is a subjective experience, a thorough and reliable assessment is vital to accurately diagnosing it and determining the most effective treatment plan. A pain assessment comprises the following components:
- a pain interview using a validated pain assessment scale
- a thorough history, including a review of all prior pain experiences, medications, and treatments
- physical examination, including a functional assessment of abilities and deficits
- psychosocial assessment
- assessment of past and current opioid use and opioid tolerance (Tauben & Stacey, 2026b)
Scales and Tools
The patient's self-report of pain severity should be evaluated using an appropriate scale, such as the Numeric Rating Scale (NRS), where 0 refers to "no pain" and 10 denotes "the worst pain imaginable." Other pain severity scales include the Visual Analogue Scale (VAS) and the Defense and Veterans Pain Rating Scale (DVPRS; Mariano, 2026). In addition, pain severity scales for individuals with verbal communication deficits related to cognitive impairment or dementia include the following:
- Faces Pain Scale (displayed in Figure 2)
- Adult Non-Verbal Pain Scale (NVPS)
- Pain Assessment in Advanced Dementia Scale (PAINAD)
The Faces scale is also widely utilized in pediatric pain assessment. Pain severity scales that allow for pain assessment using various physical features representative of pain include the Behavioral Pain Scale (BPS) and the Critical Care Pain Observation Tool (CPOT). The BPS and the CPOT are two of the most reliable, validated tools to assess pain in noncommunicative and semiconscious patients. In conjunction with the pain severity assessment scales described above, additional assessment tools help define and classify pain. The OPQRST tool is one of the most commonly used instruments. It reviews the following features of pain: onset, provocation, and palliation of symptoms, quality, region, radiation, severity, and timing (Bickley et al., 2020; Mariano, 2026; Pandharipande & Hayhurst, 2025; University of Florida [UF] Health, n.d.). An overview of the clinical use and application of the OPQRST tool is outlined in Table 4.
Figure 2
The Visual Analogue Scale, Faces Pain Scale, and Numeric Rating Scale Pain Assessment Tools
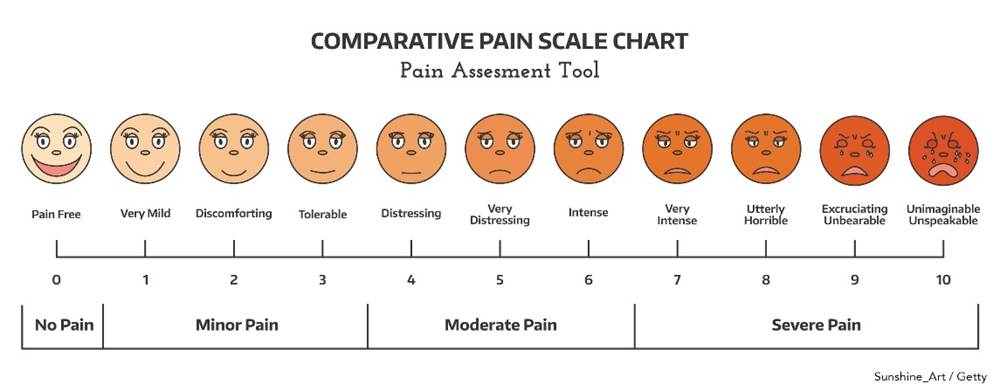
Table 4
Symptom Analysis Using the OPQRST Tool
Onset Ask the patient about the onset of the pain.
|
Provocation/Palliation of Symptoms Document associated findings: fatigue, depression, nausea, anxiety.
Aggravating/relieving factors
|
Quality Quality refers to how the pain feels: sharp, dull, aching, burning, stabbing, pounding, throbbing, shooting, gnawing, tender, heavy, tight, tiring, exhausting, sickening, terrifying, torturing, nagging, annoying, intense, or unbearable.
|
Region and Radiation Use anatomical terminology and landmarks to describe the location of pain (superficial, deep, referred, or radiating).
|
Severity Intensity, strength, and severity are “measures” of the pain.
|
Timing Timing includes the duration and frequency of the pain.
|
(UF Health, n.d.)
In addition to the above, it is helpful to ask patients about the setting of their pain, including how it affects their daily life, activities of daily living (ADLs), sleep, and school or work. Some questions to ask may include:
- “Where are you when the symptoms occur?”
- “What are you doing when the symptoms occur?”
- “How does the pain affect your sleep?”
- “How does the pain affect your ability to work or interact with others?” (UF Health, n.d.)
History and Physical Examination
The patient's medical and surgical history should be evaluated, including a detailed account of all prior trauma, injuries, and comorbid conditions. An allergy and medication history, including the use of OTC medications and supplements, is essential. The APRN should inquire about the patient’s history with prior or current pain relief measures, including pharmacological and nonpharmacological modalities, and the success or failure of each strategy. Information regarding the patient's previous experience with opioids should be explored during the initial pain assessment to determine if the patient is opioid-tolerant. It is critical to identify risks for OUD prior to opioids becoming part of the patient’s treatment plan. Behaviors complement self-report and assist in pain assessment for both verbal and nonverbal patients. Direct observation of the patient's nonverbal behavioral manifestations may indicate the presence of pain. Facial expressions (grimacing, wrinkled forehead, wincing), body movements (restlessness, pacing, guarding), and audible expressions (crying, wincing, moaning) can all indicate the presence of pain. Other physical examination findings indicating pain include decreased attention span and altered vital signs. Blood pressure, pulse, and respiratory rate increase temporarily with acute pain. However, vital signs will eventually stabilize with the persistence of pain. Therefore, physiologic indicators might not accurately measure chronic pain or pain that is present over time (Bickley et al., 2020; Pandharipande & Hayhurst, 2025; Tauben & Stacey, 2026b).
The APRN should perform a focused physical assessment related to the reported pain, including the neurological and musculoskeletal systems. In patients with clinical suspicion of neuropathic pain, signs of nerve injury may or may not be seen on the neurological exam. Some patients may demonstrate sensory deficits, including alterations in dull, pinprick, sharp touch, temperature, or vibration. Allodynia or hyperalgesia may be displayed as an exaggerated response to stimuli. Autonomic changes in the temperature and color of the extremities, as well as hair and nail growth, can accompany neuropathic pain. The patient should be evaluated for impairments in mobility, such as gait disturbance, imbalance, loss of muscle tone, reflexes, coordination, and strength (Bickley et al., 2020; Tauben & Stacey, 2026b).
Psychosocial Examination
Pain can impair many aspects of an individual’s psychological function and social well-being. The patient should be screened for the psychosocial impacts of pain, including disturbances in sleep, mood, activity, energy, appetite, and overall functioning. In addition, the patient's ability to perform ADLs, and fulfill work, or school responsibilities should be explored. Pain can also impair cognition and memory or negatively impact relationships with significant others, family, friends, and colleagues. Patients should be screened for suicidal ideation due to the increased risk with chronic pain conditions (Bickley et al., 2020; Tauben & Stacey, 2026b).
Assessment of Pain in Older Adults
It is well-cited that the incidence of pain is higher among the older adult population, who are more likely to experience pain at multiple sites. An estimated 40% of older adults have chronic pain, most commonly reported as low back pain or pain from OA (Tauben & Stacey, 2026b). Despite this, older adults receive fewer analgesics, and pain management is suboptimal. Older adults tend to report less pain than younger adults, which may be related to beliefs about pain, concerns about reporting pain, or cognitive deficits. They may underestimate their pain by attributing it to the "normal"’ aging process. Research demonstrates that many older adults believe pain must be lived with, and reporting pain is an unacceptable sign of weakness. Pain may be associated with being a "bad" patient or signify impending death or severe illness, which is therefore ignored. Fear of becoming addicted to opioids may also contribute to the older adult's reluctance to report pain. Patients and their caregivers may also be concerned about the side effects of medications or polypharmacy. Those with cognitive impairments, hearing or visual deficits, and dementia are at increased risk for undertreated pain. Special consideration should be given to the older adult population when evaluating pain. Appropriate pain scales should be utilized based on the patient’s cognitive functioning. Pain should be reassessed at each visit, and the scale should be explained each time. Attention should be paid to nonverbal indicators of pain, such as facial expressions, body movements, grimacing, guarding, and behavioral changes. In some patients, it may be helpful to avoid using the word pain and replace it with alternative verbal descriptions such as "ache," "sore," or "hurt" (Hosseini et al., 2022; Ignatavicius et al., 2024).
Developing the Pain Management Treatment Plan
An ideal pain management plan should address the etiology of pain, control current pain, and manage pain that persists despite treatment. According to HHS (2019), a pain management treatment plan should incorporate a biopsychosocial model with individualized, multimodal, and multidisciplinary strategies, integrating treatments from different clinical disciplines. A multifaceted approach to pain has been shown to enhance pain control, reducing pain severity and improving mood, overall quality of life, and functionality (HHS, 2019).
Pain treatments are evaluated based on efficacy, safety, tolerability, and invasiveness. There are two main classes of pain control: nonpharmacologic, which includes restorative therapies, interventional procedures, behavioral health approaches, and complementary therapies, and pharmacologic, which includes medications (opioid and nonopioid analgesics). Best practice guidelines recommend that pain interventions begin on the low end of invasiveness. These include psychological and physical treatments, such as restorative therapies and physical exercise programs, which will be outlined in the next section. However, the efficacy of a specific treatment does not necessarily match its degree of invasiveness (HHS, 2019).
Nonpharmacological Pain Management Strategies
Nonpharmacological strategies should not replace pharmacological pain measures; they should be used alongside them for a synergistic effect. Nonpharmacologic pain management strategies serve as a means to restore functionality, enhance comfort, reduce pain, and decrease the amount and duration of analgesics required. These strategies also help to mitigate opioid exposure when clinically indicated (HHS, 2019).
Restorative therapies include treatments provided by PT and occupational therapy (OT) professionals to promote positive clinical outcomes in various acute and chronic pain conditions. Therapeutic exercise refers to movement therapies to recover from injury, reduce inflammation, and restore health under the guidance of a trained physiotherapist. Cutaneous (skin) stimulation includes TENS therapy, heat, cold, therapeutic touch, massage, acupuncture, and acupressure. These physical modalities increase circulation, reduce pain, and are self-care alternatives to opioids. Some of the most common include:
- TENS therapy involves a small, battery-operated electric stimulator attached to the skin at the affected area(s). The device is used at home and administers a low-voltage electrical current to block the pain sensation (see Figure 3).
- Heat application causes vasodilation, promoting blood flow to the area, and is an easily accessible self-care pain relief modality. When using heating pads or other heating devices, it is essential to check the device's policy regarding how long the treatment can be safely used. In most cases, the treatment is discontinued after 15–30 minutes. When applied for over 1 hour, the body reduces blood flow to the skin through a vasoconstrictive reflex response. Dry heat applications may include aquathermia and disposable heat pads, which are most used in health care facilities. Moist heat can be applied using a lukewarm moist compress or by soaking a body part using a sitz bath. Most health care settings do not use hot water bottles since improper use can lead to burns.
- Cold application reduces swelling and helps to alleviate pain. Ice bags, collars, and gloves are applied to localized ailments. As with heat application, the device policy should be followed regarding the maximum duration the treatment may be safely used. The treatment is generally discontinued after 5–10 minutes or when the area begins to feel numb. Prolonged exposure to cold, as with heat, results in reflex vasodilation.
- Therapeutic touch is considered a pain reduction technique as it is believed to reduce pain through balance in the body. The therapist places their hands near the patient's body to balance the patient's energy field.
- Reiki is a natural healing technique in which a therapist channels energy into a patient by touch to promote physical and emotional healing.
- Massage can help reduce pain using several types of massage therapy. Swedish massage uses long strokes, kneading, and deep, circular movements; deep tissue (myofascial release) focuses on myofascial trigger points and the deeper layers of tissue. Massage stimulates circulation, relaxing the patient's muscles, reducing anxiety, and decreasing pain. Massage should be avoided when skin integrity is impaired or if infection or a blood clot is possible.
- Acupuncture and acupressure involve stimulating subcutaneous tissues using needles (acupuncture) or the digits (acupressure). Only individuals with specialized training should perform these techniques.
- Therapeutic ultrasound delivers heat and enhances blood flow to deep tissues for improved and accelerated injury healing (Berger & O’Neill, 2022; HHS, 2019; Mariano, 2026).
Figure 3
Transcutaneous Electrical Nerve Stimulation Therapy

Cognitive‑behavioral therapy (CBT) is another component of the multimodal pain management approach. It is the most recommended psychological treatment for managing chronic pain. CBT centers on developing a solid therapeutic relationship that encourages patients to adopt a problem-solving approach to cope with the challenges associated with chronic pain. It focuses on changing how patients perceive pain to reduce distress, alleviate or suppress discomfort, and improve coping skills. The overarching features of CBT include short-term, problem-focused, cognitive, and behavioral interventions. It is not a one-size-fits-all model, as there are several variations. CBT teaches patients to restructure cognitive distortions and self-defeating behaviors and replace them with more accurate thoughts and functional behaviors. CBT is time-limited and typically consists of 10–20 sessions. It can be delivered face-to-face in a clinic or via telehealth, as well as in individual or group sessions (Tauben & Stacey, 2026a). Distraction techniques direct attention toward something other than pain, as it is well-documented that decreased attention to the presence of pain can reduce the perceived pain level. Distraction techniques can be useful during painful diagnostic procedures or while waiting for an analgesic to take effect. Specific strategies include ambulation, deep breathing, visitors, television, games, prayer, and music (Berger & O’Neill, 2022).
Relaxation techniques are commonly used for pain management and may also be utilized during CBT. Relaxation strategies may include meditation, yoga, and progressive muscle relaxation. Meditation involves focusing on an object while sitting comfortably and clearing the mind of all thoughts. Meditating for 20 minutes twice daily decreases heart and respiratory rates and blood pressure. Yoga has been practiced in India for centuries and typically includes assuming poses, breathing exercises, and meditation. Yoga increases muscle strength and tone, reduces anxiety, and lowers blood pressure. Progressive muscle relaxation involves slow, deep abdominal breathing while progressively tightening and relaxing the muscles. The technique is typically performed in a logical sequence, beginning with the feet and moving up the rest of the body. Guided imagery involves pleasant and serene mental images, such as the ocean or mountains. This technique shifts the patient's thoughts away from the pain. It can be useful during painful diagnostic procedures. However, patients must be able to concentrate to benefit from guided imagery, which makes this technique more difficult for patients with acute and severe pain. Biofeedback is a therapy that uses electrical sensors to assist a patient in controlling physiological responses such as heart rate and blood pressure (Berger & O’Neill, 2022; HHS, 2019).
Interventional Pain Procedures
Interventional pain management uses minimally invasive interventions to alleviate pain and minimize pharmacological therapies. Most interventional pain procedures are performed on an outpatient basis and are, therefore, more cost-effective. Procedures vary in their degree of complexity and invasiveness. Some are considered minor procedures that can be performed in the outpatient office setting, whereas others require image guidance (using ultrasound, fluoroscopy, or computed tomography [CT]) in a radiology department. Commonly used interventional pain procedures include the following:
- Trigger point injections use dry needling or local anesthetic to inject and disrupt palpable, tense bands of skeletal muscle fibers to relax and lengthen the fibers. These may be administered intramuscularly or intrabursally (i.e., to treat bursitis).
- Joint injections use a corticosteroid and/or a local anesthetic injected into the facet joint(s) or intra-articular (such as the shoulder, elbow, wrist, knee, ankle, etc.) to manage arthritis or injury.
- Peripheral or sympathetic nerve blocks use a local anesthetic mixed with a corticosteroid. The mixture is injected or infused around a specific nerve or group of nerves to treat or diagnose postoperative pain, neuropathies, neuropathic pain, and chronic pain. An example is a celiac plexus block, which may help relieve abdominal pain related to chronic pancreatitis.
- Epidural steroid injections involve injecting corticosteroids into the epidural space (outside the dural sac in the spine) to treat neuropathic leg pain (related to a nerve root irritation in the low back) or arm pain (less common, related to a nerve root irritation in the neck).
- Radiofrequency ablation uses high-frequency energy waves (conventional or pulsed) to ablate or stun nerves contributing to pain.
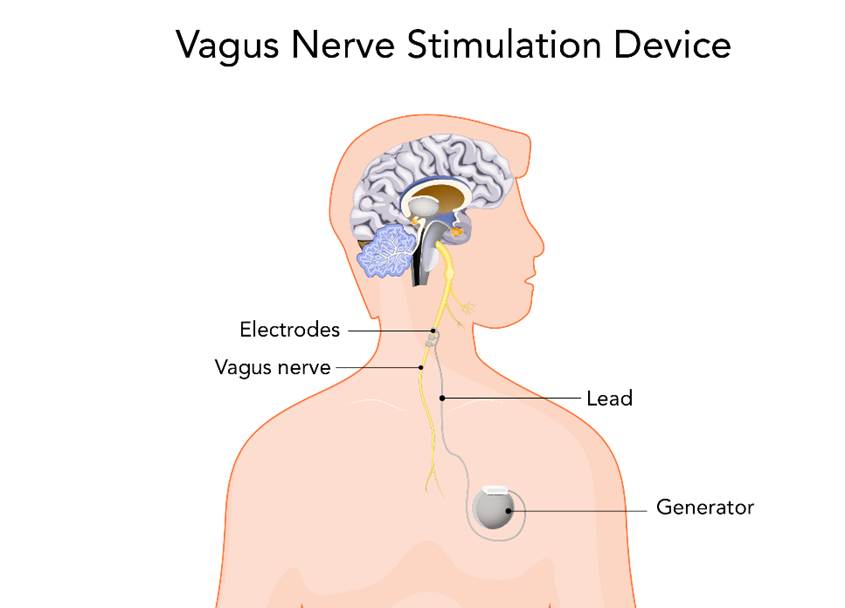
- Neuromodulation involves activating the central or peripheral nerves using electrical, ultrasound, or magnetic stimulation devices to relieve pain or reduce sensitivity. An example includes vagus nerve stimulation to treat cluster and migraine headaches (Figure 4).
- Spinal cord stimulators utilize the concept of neuromodulation (above) in a permanently implanted stimulator along the lower spinal cord to manage lower extremity neuropathic pain.
- Implanted intrathecal pain pump allows for the delivery of opioids, baclofen (Lioresal), or other medications directly into the spinal fluid to receptors on the spinal cord or the brain using a fraction of the dose required with oral administration, reducing many of the adverse drug effects. Risks include infection/meningitis, delayed respiratory depression, granuloma formation, and hypogonadism (Copenhaver et al., 2025; HHS, 2019).
Figure 4
Vagus Nerve Stimulation
Pharmacological Interventions
Pharmacologic therapy is usually a component of an effective, multimodal pain management plan, particularly for treating chronic pain, especially when there is inadequate relief with nonpharmacologic therapies. Analgesics are a mainstay for relieving pain and are composed of two main categories: nonopioids and opioids. The selection is based on the type of pain, such as neuropathic, nociceptive, nociplastic, or a mix of types (HHS, 2019; Tauben & Stacey, 2026).
Nonopioid Analgesics
Nonopioid analgesics have anti-inflammatory, antipyretic, and analgesic effects. However, the properties of the different medications vary, as each drug has its own independent mechanism of action, risks, benefits, and potential side effects. Nonopioid medications can mitigate and minimize opioid exposure (HHS, 2019).
NSAIDs
Two of the most common nonopioid analgesics are NSAIDs and acetaminophen (Tylenol). These medications are appropriate for the treatment of mild to moderate pain. They are easily accessible to patients since they do not require a prescription. Nonselective (first-generation or traditional) NSAIDs include ibuprofen (Motrin, Advil), indomethacin (Indocin), diclofenac (Zorvolex), ketorolac (Toradol), and meloxicam (Mobic). Nonselective NSAIDs inhibit cyclooxygenase (COX)-1 and COX-2, which are forms of the enzyme cyclooxygenase (COX). COX creates prostanoids (i.e., prostaglandins, prostacyclins, and thromboxanes), which are responsible for the inflammatory response. While COX-1 and COX-2 are integral to the inflammatory process, COX-1 also affects the gastrointestinal (GI) tract, kidney function, and platelet function. Therefore, when COX-1 is inhibited by nonselective NSAID therapy, inflammation, pain, and fever are reduced, but gastric ulceration, renal impairment, and bleeding can occur. COX-2 selective NSAIDS (second-generation NSAIDs or COX-2 inhibitors), such as celecoxib (Celebrex), inhibit only COX-2, decreasing inflammation, pain, and fever without impacting platelet aggregation. Although COX-2 selective NSAIDS may have a lower risk of GI adverse effects, they may have a higher risk of cardiovascular adverse effects, which is why several COX-2 selective NSAIDs are no longer on the market, leaving celecoxib (Celebrex) the only COX-2 selective NSAID on the market. The choice of NSAID depends on several other factors, including age, comorbidities, medication interactions, risk of toxicity, and half-life (Arcangelo et al., 2022; HHS, 2019; Solomon, 2024, 2025a, 2025b).
Although NSAIDs can significantly relieve many types of pain, they are not without risks. NSAIDs are associated with GI, cardiovascular, and renal effects. The most common side effects include GI bleeding, gastric ulcers, acute kidney injury, bleeding events, myocardial infarction (MI), and stroke. Not all NSAIDs pose the same severity of risk. As mentioned above, cardiovascular risks are heightened in COX-2 selective NSAIDs such as celecoxib (Celebrex); the GI side effects are reduced. Although selective NSAIDs pose less cardiovascular risk than COX-2 selective agents, they should still be used cautiously in patients with cardiovascular risk factors, as they increase the risk for MI, stroke, and heart failure exacerbation. GI risks such as bleeding, dyspepsia, and ulcers are increased in nonselective NSAID medications, including ibuprofen (Motrin) and naproxen (Naprosyn). GI risks are increased in older adults; individuals who concurrently use glucocorticoids, antiplatelet agents, and anticoagulants; individuals on high doses of NSAIDs; and individuals who have a history of GI events (Arcangelo et al., 2022; Solomon, 2026).
The American Geriatrics Society (AGS) publishes the Beers Criteria for potentially inappropriate medication use in older adults. The newest AGS Beers Criteria recommendations, released in 2023, recommend avoiding indomethacin (Indocin) and ketorolac (Toradol) due to the risk of GI bleeding, peptic ulcer disease, and kidney damage. Indomethacin (Indocin) is associated with the highest risk. Other non-COX-2 selective NSAIDs should be avoided for chronic use unless there is no other alternative option that is effective and the older adult is able to take a proton pump inhibitor (PPI) concurrently. It also states that short-term scheduled use should be avoided in older adults on corticosteroids, anticoagulants, or antiplatelet medications unless no other effective alternative option is available and the older adult is able to take a PPI concurrently. The use of concurrent PPIs reduces the risk of GI bleeding and peptic ulcer disease but does not fully eliminate it (2023 AGS Beers Criteria Update Expert Panel, 2023).
Salicylates, including aspirin, are potent inhibitors of COX-1 and COX-2 enzymes, with COX-1 being more sensitive, although their effects are less measurable in cell-free systems. Aspirin has been shown to be as effective in reducing inflammation compared to other NSAIDS in individuals with RA, despite being a weaker prostaglandin synthesis inhibitor in vitro. Aspirin affects COX-2 differently, potentially influencing cell proliferation and preventing colon cancer (Solomon, 2025a). Aspirin is also used as a primary prevention for atherosclerotic cardiovascular disease (CVD). According to the US Preventive Services Task Force (2022), the decision to start low-dose aspirin for the primary prevention of CVD in adults aged 40–59 with a 10% or higher 10-year risk of CVD should be personalized, as evidence only shows a small net benefit. They recommend against low-dose aspirin for primary prevention of CVD in adults 60 years of age and older. Lower doses of aspirin (75–81 mg/day) have an antiplatelet effect, whereas intermediate doses (650 mg to 4 g/day) have an analgesic and antipyretic effect. Regular NSAID use concurrently with aspirin for CVD prevention increases the risk of GI events. Nonsalicylate NSAID use concurrently with low-dose aspirin can also interfere with the cardiovascular benefits of aspirin (Solomon, 2026).
Salicylism poisoning is a medical emergency caused by the intentional or accidental overdose of salicylates. This potentially fatal condition develops when aspirin levels rise above the therapeutic range and can occur from the acute ingestion of large doses of aspirin at one time or from chronic intake of smaller quantities over an extended period. This results in 50–70 fatalities yearly in the United States. Early signs and symptoms of salicylism toxicity include ringing in the ears (tinnitus), nausea, and tachypnea. Moderate signs and symptoms include vomiting, mild hyperthermia, tachycardia, hyperpnea, and diaphoresis. Late signs and symptoms include confusion, hyperthermia, cerebral edema, pulmonary edema, hypertension, agitation, coma, and seizures. Salicylate poisoning has declined in children due to the recognition of Reye syndrome, limitations on tablets per bottle, and child-resistant packaging (Barnett & Boyer, 2025). Salicylates are not recommended to treat children with febrile illness due to the risk of Reye syndrome. Reye syndrome is a rapidly progressive encephalopathy that affects all body organs, being especially damaging to the brain and the liver. The most significant contributor to morbidity and mortality associated with this condition is increased intracranial pressure. Salicylate use in febrile children, specifically those with varicella and influenza A and B, is a significant precipitating factor for Reye syndrome (Chiriboga, 2025).
Acetaminophen (Tylenol)
Acetaminophen (Tylenol) is one of the most popular analgesics in the United States. The exact mechanism behind acetaminophen's (Tylenol) pain-relieving effects is not fully understood, but it is believed to work by inhibiting prostaglandin synthesis in the CNS. Because it does not inhibit prostaglandin production in the peripheral tissues, acetaminophen (Tylenol) is a weak anti-inflammatory agent. It also does not negatively impact platelet aggregation or harm the gastric lining, making it tolerated by most patients. Acetaminophen (Tylenol) is rapidly absorbed from the GI tract and reaches peak effectiveness within 1–3 hours. It is largely metabolized in the liver into inactive substances. A small portion is converted into a toxic metabolite, usually neutralized by glutathione. If glutathione levels are depleted due to chronic use or overdose, this metabolite can cause serious liver damage (Arcangelo et al., 2022). Adult dosing for pain is 325–650 mg orally every 4–6 hours as needed. Dosing for pediatric patients is 10–15 mg/kg/dose orally every 4–6 hours as needed, with a maximum of five doses in 24 hours and a maximum daily dose of 75 mg/kg/day. While doses up to 4 g/day are generally safe, there have been rare cases of liver toxicity even at lower doses. To minimize this risk, some experts suggest a maximum daily dose of 3 g for adults with normal liver function, especially if used for more than a week. For individuals with risk factors like heavy alcohol consumption, malnutrition, fasting, low body weight, older age, fever, certain liver diseases, or use of interacting medications, a lower daily dose of 2 g or complete avoidance may be advisable (UpToDate Lexidrug, n.d.-a).
While acetaminophen (Tylenol) is one of the most used analgesics in the United States, a component in hundreds of medications, and generally safe at therapeutic doses, overdose can have fatal consequences from hepatic necrosis. Acetaminophen (Tylenol) is frequently associated with drug-induced liver injury and is the leading cause of acute liver failure in the United States, responsible for half of all reported cases and about 20% of liver transplants. Patients should be encouraged to check the labels of all analgesics to determine the amount of acetaminophen (Tylenol) contained in the product. Further, frequent alcohol use while taking large doses of acetaminophen (Tylenol) heightens the risk of liver damage. Patients with preexisting liver conditions such as cirrhosis, fatty liver, or hepatitis, as well as those who consume large amounts of alcohol, should limit or avoid acetaminophen (Tylenol) as much as possible. Other factors that increase the risk of hepatotoxicity include older age, genetic factors, nutritional status, and ingestion of other drugs. Diagnosis is characterized by marked elevations in plasma aminotransferases (liver enzymes) and rising prothrombin time/international normalized ratio (PT/INR; Burns et al., 2024). Diagnosis is confirmed by an elevated serum acetaminophen concentration. The clinical course of acetaminophen (Tylenol) poisoning moves through four sequential stages as follows:
- Stage I (30 minutes to 24 hours): nausea, vomiting, lethargy, diaphoresis, and pallor
- Stage II (24–72 hours): laboratory evidence of hepatotoxicity and nephrotoxicity becomes apparent, including hyperbilirubinemia, elevated PT, and clinical manifestations such as right upper quadrant (liver) pain, tenderness, and hepatomegaly
- Stage III (72–96 hours): elevations in liver function enzyme tests peak by 96 hours (plasma alanine transaminase [ALT] and aspartate aminotransferase [AST] levels may exceed 10,000 IU/L), hyperbilirubinemia (bilirubin usually exceeds 4.0 mg/dL), and clinical manifestations such as jaundice, confusion (hepatic encephalopathy), bruising or bleeding, oliguria, and multiorgan system failure ensue. Death most commonly occurs during stage III
- Stage IV (4 days to 2 weeks): patients who survive stage III enter a recovery phase that usually begins on the fourth day following the overdose. Patients often develop chronic liver changes, including necrosis and chronic liver disease, and may eventually need a liver transplant (Burns et al., 2024)
GI decontamination with activated charcoal (AC) is recommended for patients who present within 4 hours of potentially toxic acetaminophen (Tylenol) ingestion (i.e., a single dose of 7.5 g or greater). AC is a gastric lavage technique that induces emesis, limiting acetaminophen (Tylenol) absorption and reducing the need for acetylcysteine (Acetadote) treatment. Acetylcysteine (Acetadote) is the antidote for acetaminophen (Tylenol) overdose/poisoning and should be given to all patients at significant risk for hepatotoxicity. Severe hepatotoxicity is uncommon, and death is rare when this antidote is administered within 8 hours of overdose. Acetylcysteine (Acetadote) decreases the build-up of hepatotoxic metabolites to prevent or lessen liver damage. It can be given orally or intravenously, and several protocols for administration are available and vary according to institution policy and patient tolerance (Heard & Dart, 2025).
Antiseizure Medications
Antiseizure medications were initially developed to treat seizures but are also commonly used to treat specific pain syndromes. As mentioned, these drugs are particularly effective for treating neuropathic pain and migraines. Increasingly, they are being incorporated into a multimodal approach to managing perioperative pain to reduce the need for opioids postoperatively. Gabapentinoids such as gabapentin (Neurontin) and pregabalin (Lyrica) are commonly prescribed for chronic neuropathic pain such as PHN, diabetic neuropathy, and fibromyalgia (HHS, 2019). They act as inhibitors of voltage-gated calcium channels and suppress neuronal excitability, which makes them optimal analgesics for neuropathic pain. The initial dosing of gabapentin (Neurontin) is typically 300 mg at night, with a typical effective dose of 1,200–2,400 mg/day divided into three doses. The maximum dose is 3,600 mg. There is also an extended-release (ER) option that is typically started at 300 mg/day and increased to a maximum of 1,800 mg/day for efficacy. Pregabalin (Lyrica) is like gabapentin (Neurontin) but contains a different active ingredient and has more stable pharmacokinetics; thus, it is dosed twice daily instead of three times per day. The typical starting dose of pregabalin (Lyrica) is 50 or 75 mg once at night, then increased to 150–450 mg/day. Increased titration to a maximum of 600 mg/day may be needed. Asymmetrical dosing, with a larger dose at night, may help with sleep. Although gabapentin (Neurontin) and pregabalin (Lyrica) effectively treat nerve pain, they have several side effects, including sedation, fatigue, dizziness, visual disturbance, mood swings, depressive episodes, and suicide attempts. Because they are known to increase the risk of suicidal thoughts or behavior, these medications should be used cautiously in patients with concomitant psychiatric conditions or those with a history of depression, suicidal thoughts, ideation, or attempt. Patients and caregivers should be counseled on monitoring for mood changes, such as new or worsening depression, anxiety, restlessness, panic attacks, anger, irritability, agitation, aggression, dangerous impulses, violence, and suicidal thoughts or behaviors (HHS, 2019; Schwenk, 2025; Tauben & Stacy, 2025).
As mentioned earlier, carbamazepine (Tegretol) or oxcarbazepine (Trileptal) is recommended as initial medical management of TN. These have been shown to provide relief in up to 90% of patients with this condition. Carbamazepine (Tegretol) inhibits voltage-gated sodium channels, reduces the excitability of neural membranes, and potentiates GABA receptors. The usual starting dose of carbamazepine (Tegretol) is 100 to 200 mg twice daily, increased by 200 mg every 1–2 weeks until sufficient pain relief or intolerable adverse effects prevent further upward titration. The standard maintenance dose for TN pain is 600–800 mg daily, administered in two or four divided doses depending on the form. The maximum suggested daily dose is 1,200 mg. It must be used with caution in patients on cancer chemotherapy, which can cause bone marrow suppression, because it can additionally induce leukopenia. The most common adverse effects include dizziness, sedation, disturbances in concentration, ataxia, and visual disorders such as diplopia. Other potentially severe but uncommon adverse effects include Stevens-Johnson syndrome, systemic lupus erythematosus, toxic epidermal necrolysis, hepatotoxicity, hyponatremia, and aplastic anemia. Routine laboratory monitoring, including complete blood count, serum sodium, and liver function tests, should be performed to monitor for these serious adverse effects. In addition, patients should be educated on the importance of avoiding grapefruit or grapefruit juice while taking carbamazepine (Tegretol), as it inhibits the drug’s metabolism and can increase adverse effects. Oxcarbazepine (Trileptal) may be better tolerated and has fewer noted drug interactions. It is dosed at 150–300 mg twice daily with increases of 300 mg every 3 days, totaling 1,200–1,900 mg daily. Adverse effects are similar to carbamazepine (Tegretol). Before starting either of these medications in genetically at-risk populations (i.e., East Asian or South Asian), testing for the HLA-B*15:02 allele is recommended. Patients with one copy of this allele have an increased risk of Stevens-Johnson syndrome and/or toxic epidermal necrolysis and should not be started on these medications (Ho et al., 2026; NINDS, 2026b).
Topical Analgesics
Topical agents have some advantages over systemic medications, such as fewer systemic effects and the ability to deliver directly to the site of pain. They are used for nociceptive or neuropathic pain that is well-localized. While they may be used alone as first-line therapy, they are often used as an adjunct to other systemic drugs. Topical agents include NSAIDs, lidocaine, and capsaicin (Capsagel). Topical NSAIDs come in several forms (i.e., gel, spray, cream) and are often beneficial for OA in a single joint. Although systemic effects are possible with topical agents, topical NSAIDs are less likely to cause GI, renal, and cardiovascular toxicity. The most common side effect of topical NSAIDs is a mild skin rash. An example of a topical NSAID is diclofenac topical gel (Voltaren Arthritis Pain). The usual dose is 4 g of gel to the affected area three to four times per day (Tauben & Stacey, 2025).
Topical lidocaine is a second-line therapy for neuropathic pain and is typically used in patch or plaster form. While the data on its efficacy is limited, it may help with PHN and diabetic neuropathy. Three patches can be applied at one time, but each patch should only be applied for up to 12 hours, with a 12-hour free period. Systemic absorption rates are low, but topical lidocaine should be used with caution in individuals with renal, hepatic, or cardiac conditions. A lidocaine patch (5%; Lidoderm) has 700 mg of lidocaine. These are also most useful for local pain relief, such as PHN, but should only be used on intact skin. Topical lidocaine cream (5%; NumbCream) should be applied in a thin layer three to four times a day, with a maximum of six times (Tauben & Stacey, 2025).
Capsaicin (Capsagel, Salonpas) is a topical analgesic derived from chili pepper extract, a neuropeptide-releasing agent that targets peripheral sensory neurons. It is applied to the skin to control peripheral nerve pain, and its benefits in managing chronic neuropathic pain have been widely studied. It is commonly used in HIV neuropathy, PHN, diabetic neuropathy, and OA. Lower concentration forms are available primarily OTC as a gel, cream, or lotion. These should be applied three to four times per day over the affected area for a maximum of 6–8 weeks. Higher concentration forms include patches by prescription. These must be administered by a healthcare professional and are applied for 30–60 minutes and repeated up to every 3 months. Pretreatment with lidocaine or a stronger analgesic is recommended prior to patch administration, and patches are commonly used for diabetic neuropathic pain and PHN. The main adverse effects are stinging, burning, and site erythema, which leads to intolerance in some patients (Tauben & Stacey, 2025).
Tricyclic Antidepressants
TCAs help reduce neuropathic pain and various other chronic pain conditions. Despite no TCAs having FDA approval for use in pain management, they are often used for this indication in patients with and without depression. They have independent analgesic properties and are also known to potentiate the effects of opioids. These medications block the reuptake of serotonin and norepinephrine at the synapse in the brain, which helps improve mood and treat depression. For pain, they act on the descending pain pathways involving serotonin, norepinephrine, and endogenous opioids. Amitriptyline (Elavil) is the most commonly used TCA in pain management. Others include doxepin (Silenor), imipramine (Tofranil), nortriptyline (Pamelor), and desipramine (Norpramin). Amitriptyline (Elavil) is the only TCA with proven efficacy for migraines. Although TCAs are widely studied for their benefits in relieving pain, they are associated with several adverse effects, which make tolerance difficult. Some of the most common include orthostatic hypotension, dry mouth, dizziness, weight gain, memory impairment, urinary retention, constipation, sedation, tachycardia, and cardiac conduction abnormalities (particularly QTc interval prolongation; Arcangelo et al., 2022; Tauben & Stacey, 2025).
TCAs should be initiated at low doses and gradually titrated upward as tolerated to achieve optimal effect. For example, the starting dose of nortriptyline (Pamelor) is 10 mg daily, with an increase of 10–25 mg at weekly intervals, and the maintenance dose is up to 150 mg daily. Patients should be advised to take the medication at bedtime to minimize the effects of orthostatic hypotension and sedation. Nortriptyline (Pamelor) is associated with less sedation and fewer anticholinergic side effects than other TCAs. These medications are not recommended as first-line agents in pain management. Additionally, abrupt discontinuation of TCAs is associated with withdrawal symptoms, such as nausea, anxiety, and insomnia (Arcangelo et al., 2022; Tauben & Stacey, 2025).
SNRIs
Duloxetine (Cymbalta), milnacipran (Savella), and venlafaxine (Effexor) are SNRIs used to treat neuropathic pain and fibromyalgia. They are often tolerated better than TCAs. Duloxetine (Cymbalta) has shown efficacy for improving function, sleep, and quality of life in individuals with chronic pain modestly. It is FDA-approved for chronic musculoskeletal pain, diabetic neuropathy, and fibromyalgia. Milnacipran (Savella) has also been shown to provide modest pain relief, but with less evidence than duloxetine (Cymbalta). It is FDA-approved for fibromyalgia. Standard doses of SNRIs are typically as effective in pain management as higher doses, though higher doses may help some patients, but require close monitoring. The starting dose of duloxetine is 30 mg daily for 1 week and then increasing to 60 mg daily if indicated. Some patients may be initiated on 20 mg, and others may be increased to doses as high as 120 mg daily for maximal analgesic effect. Common side effects include nausea and dizziness, and it should be avoided in patients with liver or severe kidney issues. Milnacipran (Savella) is more potent in norepinephrine reuptake inhibition, and venlafaxine (Effexor) acts like a selective-serotonin reuptake inhibitor (SSRI) at low doses but has increased norepinephrine reuptake at higher doses. It should be used cautiously in patients with cardiac issues due to potential conduction abnormalities and blood pressure increases. Discontinuation symptoms are common due to their shorter half-life; however, tapering all SNRIs is recommended to prevent withdrawal. A benefit of these medications is their concurrent effect on mood disorders. As with all antidepressants, patients must be assessed for suicidal thoughts or ideations before starting therapy and reassessed throughout treatment (Arcangelo et al., 2022; Tauben & Stacey, 2025; UpToDate Lexidrug, n.d.-b, n.d.-c).
Glucocorticoids
Glucocorticoids, otherwise known as corticosteroids, reduce pain by decreasing inflammation. They are efficacious in treating painful inflammatory conditions such as RA and gout. Some of the most common agents include dexamethasone (Decadron), methylprednisolone (Medrol Dosepack), and prednisone (Deltasone). Long-term systemic corticosteroid use can lead to several adverse effects, including hyperglycemia, bone loss, skin thinning, cataracts, weight gain, elevated glucose, immunosuppression, and adrenal insufficiency. Corticosteroids can also cause mood and behavioral changes, including irritability and aggression. Therefore, these medications are not advised for long-term use and should be tapered down as soon as possible. Due to the risk of adrenal insufficiency and withdrawal symptoms, corticosteroids should not be discontinued abruptly or tapered down too quickly. Withdrawal symptoms include weakness, severe fatigue, body aches, lightheadedness, and irritability (Berger & O’Neill, 2022).
Bisphosphonates
Bisphosphonates, such as alendronate (Fosamax) and ibandronate (Boniva), are typically indicated for the prevention and treatment of osteoporosis. Specific medications, such as denosumab (Xgeva) and zoledronic acid (Zometa), are also used for cancer-related bone pain from bone metastases or primary bone cancer. They inhibit osteoclast cell activity, decrease bone turnover, and increase bone density. Bisphosphonates carry serious risks, including irritation of the upper GI tract, hypocalcemia, medication-related osteonecrosis of the jaw (MRONJ), and atypical femur fracture (AFF). Their use is contraindicated in patients with hypocalcemia, esophageal stricture, upper GI disease, and severe renal dysfunction (i.e., creatinine clearance less than 35 mL/minute). Before starting bisphosphonate therapy, patients should be educated about the risks and warnings associated with its use. They should have a prophylactic dental evaluation and follow up regularly with their dentist during treatment (Camacho et al., 2020; Yu & Hoffe, 2025).
Muscle Relaxants
In general, muscle relaxants are not recommended to treat pain. Muscle relaxants, such as methocarbamol (Robaxin) and metaxalone (Skelaxin), do not directly relax muscles and may work through sedation. If true spasticity is present, then an antispasticity drug is recommended. Muscle relaxants can cause CNS depression and should be used cautiously, especially in older adults or with other medications that may cause CNS depression. Muscle relaxants may be used as a second-line therapy for the treatment of acute low back pain in patients who do not respond to initial therapy with NSAIDs or acetaminophen (Tylenol). They should not be used as initial therapy due to side effects. Cyclobenzaprine (Flexeril) is often a first choice, with pharmacologic properties similar to TCAs. It may provide short-term relief for those with acute low back pain. The most common adverse effects are sedation and dizziness. Misuse and dependence are concerns with benzodiazepine muscle relaxants. Carisoprodol (Soma) is not recommended for any indication due to its risks of dependence, adverse effects, and lack of proven efficacy. Cyclobenzaprine (Flexeril) may also be used for mild to moderate fibromyalgia symptoms (Knight & Chou, 2026; Tauben & Stacey, 2025).
Cannabinoids
Treatment of pain with cannabinoids is complicated and can be controversial due to laws across the United States and different states. The active compound in cannabinoids that is thought to have an analgesic effect is delta-9-tetrahydrocannabinol (THC). It is important for APRNs to have knowledge of cannabinoids and their use for pain, as patients may seek recommendations in states where it is legal for recreational and medical use. A trial may be reasonable in patients with failed trials of other medications, only in patients with no history of SUD, and those with realistic expectations. The benefits should be weighed against the risk of harm, and cannabinoids should not be routinely prescribed with other high-risk pain medications such as opioids. Patients should all be educated about the safety of driving and operating heavy equipment when taking cannabinoids. Adverse effects may include dizziness, dry mouth, nausea, drowsiness, hallucinations, and euphoria (Tauben & Stacey, 2025).
Benzodiazepines
Benzodiazepines have been prescribed to treat anxiety accompanying pain. However, there is no evidence of efficacy for their use in treating pain. Additionally, they are not first-line treatments for anxiety or sleep. They have a high risk for misuse, addiction, and respiratory depression, especially with concomitant opioid use, and they create an increased rate of all-cause mortality. Their use with opioids in those with noncancer pain may result in worse pain, higher opioid prescriptions, higher rates of substance use, and more co-occurring mental health conditions (Tauben & Stacey, 2025).
Emerging Nonopioid Therapies
Ketamine (Ketalar) is an emerging therapy for acute pain, as well as complex regional pain syndrome, neuropathic pain, and other chronic pain conditions, but there is still little evidence to support its use. It is used to treat depression and suicidal ideation, and the analgesic effect may be partially related to improved mood. Liver function should be evaluated prior to administration due to the risk of hepatobiliary dysfunction. Ketamine (Ketalar) is not recommended for standalone therapy and should be used as part of a comprehensive plan in consultation with other experts. Lidocaine infusion is another emerging therapy used for perioperative pain and chronic neuropathic pain, although it also does not yet have convincing evidence to support its use (Tauben & Stacey, 2025).
Opioid Prescribing and Monitoring
In light of the opioid epidemic plaguing the United States, APRNs must ascertain an accurate and comprehensive understanding of best practices for opioid prescribing and monitoring to preserve the integrity of clinical practice, safeguard patient care, and reduce the risk for OUD. It is vital that APRNs properly understand terms related to opioid use, such as tolerance, dependence, and addiction, as there are many misconceptions related to these concepts, which may contribute to the inadequate treatment of pain (Berger & O’Neill, 2022; Dowell et al., 2022). Key concepts associated with opioid use are defined in Table 5.
Table 5
Terminology Associated with Opioid Use
Term | Definition |
Tolerance | Tolerance is a state of adaptation in which exposure to an opioid induces changes that decrease one or more of the drug's biological effects over time. As a result, the individual requires higher doses of the medication over time to maintain the same level of response or effects. |
Physical and psychological dependence | Physical dependence is the body's physical adaptation to a drug. The medication becomes necessary for normal body functioning, and symptoms of withdrawal develop when the drug is no longer present in the patient's body; this can be caused by abrupt cessation or rapid dose reduction of the drug or the administration of an antagonist (i.e., naloxone [Narcan]). Psychological dependence occurs when ingesting the medication becomes associated with alleviating pain, anxiety, or depression. The presence of the drug becomes a calming and reassuring presence in the patient's life, similar to a comfort or security object Signs of dependence include:
|
Addiction | Addiction is a chronic, neurobiological disease that has contributing genetic, psychosocial, physical, and environmental factors and influences, manifested by behaviors that include one or more of the following:
|
Pseudotolerance | Pseudotolerance is the misconception that increasing doses are needed due to tolerance rather than disease progression or other factors. |
Pseudoaddiction | Pseudoaddiction is the faulty assumption of addiction in a patient seeking relief from pain. It is manifested by a patient becoming intensely fearful of being in pain. Pseudoaddiction is common in postoperative patients and usually manifests as clock-watching, asking to be awoken to receive pain medication, and hypervigilance with documenting and monitoring pain medication administration. Pseudoaddiction usually resolves with effective pain management treatments and the resolution of painful stimuli; for postoperative patients, this is the healing of the surgical site. |
Misuse | Misuse is the nonmedical use of opioids and is characterized by taking an opioid in a manner or dose other than prescribed (e.g., taking the drug to get high or taking someone else's prescription). |
Prescription drug diversion | Prescription drug diversion is the unlawful channeling of regulated pharmaceuticals from legal sources to the illicit marketplace; legitimately made controlled substances that are diverted from their lawful and medically necessary purpose into illegally trafficked drugs. |
(Berger & O’Neill, 2022; CDC, 2024b; HHS, 2019)
Opioids
Opioids are a group of controlled-substance analgesics prescribed for moderate to severe pain. Compelling evidence does not suggest their routine use for patients with chronic pain, and their use should be at the lowest effective dose, for the shortest time, and with frequent risk assessment. Opioids can be natural (derived from the opium poppy plant), synthetic (human-made), or semisynthetic. They interact with opioid receptors on nerve cells to reduce pain signals and sensation by binding to and activating opioid receptors (i.e., mu, delta, and kappa), which are widely distributed throughout the CNS. Attaching to one of these receptors reduces or blocks pain signals sent from the brain to the body, releasing dopamine throughout the body, thereby altering pain perception and response. Opioids can also affect receptors in the respiratory and GI tract, leading to occasional use for diarrhea and cough. Opioids are classified as agonists, partial agonists, and mixed agonist-antagonists. Opioid antagonists may be used to counteract the adverse effects of opioids. Although opiates and opioids may be used interchangeably, they have different meanings. Opiates include natural opioids such as heroin, morphine, and codeine, whereas opioids include all-natural, synthetic, and semisynthetic opioids such as oxycodone (Roxicodone) and fentanyl (Duragesic; Berger & O’Neill, 2022; CDC, 2024b; NIDA, 2021).
Opioid Agonists
Opioid agonists produce a maximum biological effect between receptor binding and response. Opioids vary in the ratio of their analgesic potency and their potential for respiratory depression (Berger & O’Neill, 2022). Adverse reactions to opioid agonists include respiratory depression, drowsiness, mental confusion, nausea/vomiting, dizziness, headache, fatigue, pruritus, pinpoint pupils, urinary retention, and constipation. Since opioids induce euphoria, particularly when taken in higher doses than prescribed or ingested via snorting or injection, they carry an increased risk for abuse and addiction. In addition, long-term opioid use poses an increased risk of drug tolerance and hyperalgesia from damage to nociceptors. Opioid agonists for moderate or severe pain include:
- Hydrocodone (Vicodin, Lortab, Norco): found only in combination products, usually combined with acetaminophen (Tylenol); may be an oral tablet formulation or a liquid cough syrup
- Oxycodone (Roxicodone, Oxycontin): available as an immediate-release (IR) or extended-release (ER) formula, fast onset, available in oral tablet or solution form
- Morphine sulfate (Roxanol, MS Contin): available as an IR or ER formula in parenteral and oral formulations
- Oxymorphone (Opana, Opana ER): available as an IR or ER formula, long half-life in parenteral and oral formulations
- Hydromorphone (Dilaudid, Exalgo ER): derivative of morphine, but with a faster onset, available as an IR or ER formula in oral tablet, liquid, suppository, and parenteral preparations (HHS, 2019; NIDA, 2021; Portenoy et al., 2024)
Some of the most common opioid agonists are listed according to their origins in Table 6.
Table 6
Opioid Analgesics
Natural | Synthetic | Semisynthetic |
Morphine sulfate (Roxanol, MS Contin) | Fentanyl (Duragesic) | Oxycodone (Roxicodone) |
Codeine (Tylenol #3) | Hydrocodone (Vicodin) | |
Meperidine (Demerol) | Hydromorphone (Dilaudid) | |
| Tramadol (Ultram) | Oxymorphone (Opana) |
Buprenorphine (Butrans) |
(Berger & O’Neill, 2022; CDC, 2024b)
Fentanyl (Duragesic) is a highly lipid-soluble opioid administered through various parenteral modalities, including transdermal, transmucosal, intranasal, spinal, and intravenous via patient-controlled devices. Fentanyl dosing is in micrograms due to its high potency; it is 50–100 times more potent than morphine sulfate (Roxanol, MS Contin). Methadone (Dolophine) is a long-acting (LA) opioid used for neuropathic pain and OUDs. The half-life of methadone (Dolophine) is significantly longer than that of morphine (8–59 hours), with lipophilic storage, so caution is advised when using this drug to treat pain safely. This prolonged plasma half-life allows longer dosing intervals. Prescribers must have skill and experience in prescribing this drug. However, it is considerably cheaper than other medications and is widely dispensed in SUD clinics as a component of medication-assisted treatment (MAT) for OUD. Since it is LA, it can delay the opioid withdrawal symptoms that patients experience when taking short-acting opioids, allowing time for detoxification. Codeine is a relatively weak opioid agonist commonly used to treat mild to moderate pain. It can be administered alone, combined with acetaminophen (Tylenol-Codeine #3), or as part of cough and cold formulas (Arcangelo et al., 2022; HHS, 2019; Portenoy et al., 2026; Rosenquist, 2025).
Partial Agonists
Partial agonists activate opioid receptors to a lesser degree than full agonists. Low doses provide similar effects to full agonists, but the analgesic activity plateaus when the doses are increased; thus, they have a ceiling effect. Therefore, increasing dosages of these medications typically lead to more adverse effects without improved pain relief. Examples of partial agonists include tramadol (Ultram) and buprenorphine (Suboxone). Tramadol (Ultra) is a synthetic analog of codeine with a low affinity for opioid receptors, commonly used to treat moderate to severe pain. It has a dual mechanism of action and poses less abuse potential than other opioids. It is available in IR or ER oral formulations, with the ER used more commonly for chronic pain. Adverse effects include dizziness, vertigo, nausea, constipation, and headache (Berger & O’Neill, 2022).
Buprenorphine (Suboxone) is a semisynthetic partial agonist used in MAT to treat OUD. It has unique pharmacological properties that help reduce the potential for misuse and diminish the effects of physical dependency on opioids, including withdrawal symptoms and cravings. Similar to opioids, it can lead to euphoria and respiratory depression when administered at low-to-moderate doses; however, these effects are weaker than with full opioid agonists. Therefore, buprenorphine (Suboxone) increases patient safety during overdose. It was first approved for use by the FDA in 2002, in combination with counseling and behavioral therapies to treat OUD. There are several types of FDA-approved buprenorphine (Suboxone) products, including buprenorphine/naloxone (Bunavail) buccal film, buprenorphine/naloxone (Zubsolv) sublingual tablets, and buprenorphine ER injection (Sublocade). The advantage of buprenorphine (Suboxone) over methadone (Dolophine) is that it does not require close monitoring in the highly structured environment of methadone clinics. Since buprenorphine (Suboxone) is an LA agent, most patients do not require daily dosing. The opioid effect of buprenorphine (Suboxone) increases with the dose until it levels off with moderate doses. This "ceiling effect" helps to lower the risk of misuse, dependency, and side effects. Common side effects of buprenorphine (Suboxone) include nausea, vomiting, constipation, muscle cramps, inability to sleep, cravings, distress, irritability, and fever (Strain, 2026). The Consolidated Appropriations Act, 2023, removed the federal requirement for prescribers to have a special waiver to prescribe buprenorphine (Suboxone) for OUD. Now, all prescribers with Schedule III authority can prescribe it for this use (Substance Abuse and Mental Health Services Administration [SAMHSA], 2024).
There are two preparations of buprenorphine that are now approved by the FDA for severe pain. These include buccal and transdermal. They are indicated when around-the-clock opioid therapy is indicated, and alternative therapies have not adequately relieved pain. The formulas for OUD are often combined with naloxone (Narcan), whereas those used for chronic pain are not combination formulations. The dose for severe pain is usually less than that for OUD. The starting dose for buccal film is 75 mcg. Its advantages for pain management include less association with hyperalgesia and less risk of respiratory depression. However, as noted above, it is still associated with several adverse effects (Rosenquist, 2025).
Mixed Agonist-Antagonists
An agonist-antagonist is an opioid that has mixed actions. These drugs produce different effects at various receptors, acting on one opioid receptor to create a response and binding to another receptor to prevent a response. Medications in this class demonstrate varying activity depending on the target receptor and the drug dose. Common agonist-antagonists include pentazocine/naloxone (Talwin) and butorphanol (Stadol). Pentazocine/naloxone (Talwin) is a combination agent for moderate to severe pain. It acts by binding to and activating specific opioid receptors while simultaneously blocking the activity of other opioid receptors. The naloxone (Narcan) component of the medication helps to prevent misuse. Butorphanol (Stadol) is a mixed opioid agonist-antagonist available as a spray for treating migraine headaches. Similar to partial agonists, agonist-antagonist opioids have a ceiling effect. As a result, increased dosages offer lower analgesic efficacy and a higher risk for psychotomimetic or psychotogenic effects (e.g., hallucinations and delirium; Berger & O’Neill, 2022).
Opioid Antagonists
Opioid antagonists compete with opioids at receptor sites to reverse the acute adverse effects, primarily respiratory depression, caused by opioids or to treat OUD. The two most common opioid receptor antagonists are naloxone (Narcan) and naltrexone (Vivitrol). Naloxone (Narcan) is the most widely used opioid antagonist, as it is FDA-approved for acute opioid overdose. Naloxone (Narcan) is highly effective in reversing opioid overdose and respiratory depression. It is dispensed in various formulations (e.g., intravenous, intramuscular, subcutaneous, and intranasal). When administered intravenously, effects begin almost instantly and last for about an hour. The dose should be titrated to reverse respiratory depression without fully reversing the analgesic effects. Rapid medication infusion should be avoided to reduce the risk of hypertension, tachycardia, nausea, and vomiting. Vital signs should be monitored, especially respirations, and naloxone (Narcan) administration should be repeated until the manifestations of opioid toxicity have subsided. With intramuscular, subcutaneous, and intranasal administration, the drug takes effect in 2–5 minutes and lasts several hours. These administration routes are most commonly used by emergency medical services (EMS) personnel and civilians responding to opioid overdose in the community (CDC, 2025b; Stolbach & Hoffman, 2026; Theriot et al., 2026).
According to the CDC (2025), approximately 80,000 drug overdoses in 2023 were a result of opioids, and a bystander was present in about 43% of these overdoses involving opioids. Thus, the opioid epidemic has led to the widespread use of naloxone (Narcan) among EMS personnel and persons in the community. Bystanders can act to prevent overdose deaths as naloxone (Narcan) is now available across the country (CDC, 2025b). The prescribing and dispensing of naloxone (Narcan) have become a central part of the public health response to the opioid overdose epidemic. Most states allow naloxone (Narcan) to be purchased from a pharmacy without a prescription. In 2023, the FDA approved it for OTC use. The nasal spray is a prefilled device that delivers 4 mg of the medication into one nostril or 1 mg in each (see Figure 5). This may be repeated every 2–4 minutes until the patient becomes responsive. The injectable formulation is injected into the muscle or under the skin (see Figure 6). Prefilled syringes with 5 mg per 0.5 mL or 1 mg/mL may be repeated every 2–3 minutes as above. Intranasal administration has several advantages over injectable formulations when responding to overdose patients in the community. The safety profile of intranasal formulations appears to be equivalent to injectable formulations for treating opioid overdose (CDC, 2025b; Coffin, 2026; Stolbach & Hoffman, 2026).
Figure 5
Naloxone (Narcan) Nasal Spray

Figure 6
Prefilled Syringe of Naloxone (Zimhi) Injectable

Prescribers are advised to consider providing a concurrent prescription for naloxone (Narcan) for patients at high risk for intentional or accidental overdose. According to the CDC 2022 Opioid Prescribing Guidelines, if a patient’s opioid dosage reaches or exceeds 50 morphine milligram equivalents (MME)/day, clinicians should implement additional precautions, including increased frequency of follow-up and prophylactic naloxone (Narcan) with overdose prevention education to both the patient and the patient’s household members (Dowell et al., 2022; Rosenquist, 2025). Patients at the highest risk include those who meet any of the following criteria:
- doses of >90 MME per day
- chronic opioid use
- concurrent use of benzodiazepines
- personal history of SUD/OUD
- current treatment for substance abuse/opioid misuse disorders
- family history of SUD
- patients who live in isolated or rural areas
- patients with chronic respiratory, renal, hepatic, or cardiac disease or HIV/AIDS
- current or history of depression or other severe mental health conditions (Coffin, 2026; Dowell et al., 2022)
Serious adverse effects of naloxone (Narcan) are rare, and usually, the benefit of using it for an overdose outweighs the risk for adverse effects. However, it can induce acute opioid withdrawal symptoms such as tachycardia, agitation, vomiting, body aches, and convulsions. Naloxone has no reversal effect on alcohol or other CNS depressants such as benzodiazepines (Coffin, 2026).
Naltrexone (Vivitrol) is FDA-approved to treat opioid dependence and alcohol use disorder. Naltrexone (Vivitrol) binds to and blocks opioid receptors to suppress opioid cravings. It is not used to treat acute opioid overdose. Patients must detox from opioids before starting naltrexone (Vivitrol); they must be opioid-free for at least 7–10 days to prevent opioid withdrawal syndrome. When used for OUD, its purpose is to prevent euphoria and the desire to use opioids. Naltrexone (Vivitrol) is also used to reverse postoperative respiratory depression due to opioid use during the operative period. Naltrexone (Vivitrol) is available in oral, intramuscular, and implantable formulations. Implants are not yet available in the United States. Naltrexone (Vivitrol) has an extensive first-pass effect; following oral administration, the half-life is 4 hours. Following intramuscular administration, the half-life is 5–10 days. For OUD, naltrexone (Vivitrol) should be started at 25 mg once daily for a few days and then increased to 50 mg once daily. The intramuscular injection is administered monthly. Any licensed prescriber can prescribe naltrexone (Vivitrol) without a specific license or training requirement (Singh & Saadabadi, 2023; Theriot et al., 2026).
Opioid Routes of Administration
Opioids can be administered via oral, intravenous, intramuscular, transdermal, and subcutaneous routes. They are supplied in short-acting and LA preparations. Regardless of the route of administration, education regarding the adverse effects, risks, and benefits is vital in understanding clinical indications and patient outcomes. Oral administration of analgesics is generally preferred for patients whenever possible due to ease of administration, cost-effectiveness, and monitoring. However, the duration of action for most short-acting oral opioids is only about 4 hours. ER formulations usually provide pain control for 8–12 hours or more. Intranasal analgesic administration is advantageous because the medication is rapidly absorbed. Topical analgesics are applied directly to the skin and are absorbed by vascular uptake. This route may reduce pain during a painful procedure, such as a lumbar puncture. Due to its rapid onset, lidocaine (Lidocaine viscous) is commonly used for dental procedures or other superficially invasive procedures such as skin biopsies. The transdermal analgesic route may also be used to treat chronic pain. LA topical medication can control pain for several hours to days. Transdermal fentanyl (Duragesic) is indicated for patients who have severe pain and are opioid-tolerant (Berger & O’Neill, 2022).
The transmucosal analgesic route is frequently used for hospice patients experiencing breakthrough pain. The oral mucosa is highly vascular, providing rapid absorption. The rectal route for administering analgesics can also be used when immediate pain control is desired as the rectal mucosa is highly vascular, allowing rapid absorption of the medication. This route is helpful for unconscious patients, those who have difficulty swallowing, or who are experiencing nausea and vomiting. When epidural analgesia is used, an anesthesiologist or nurse anesthetist inserts a catheter into the epidural space along the spine. An analgesic such as morphine (Roxanol, MS Contin) or fentanyl (Duragesic) is infused through the catheter. The patient should be monitored closely for respiratory depression, excessive sedation, hypotension, bradycardia, and urinary retention. The use of other opioids or CNS depressants should be avoided during the use of epidural analgesia. The health care team should closely monitor the patient and be prepared to administer naloxone (Narcan) for symptoms of respiratory depression or excessive sedation (Berger & O’Neill, 2022).
Patient-Controlled Analgesia (PCA)
PCA is a medication delivery system that allows patients to self-administer safe doses of opioids and is almost exclusively used in acute inpatient hospital and inpatient hospice settings. Some fundamental principles regarding the use of a PCA are summarized in the bullet points below.
- A PCA provides small, frequent dosing to ensure consistent plasma levels.
- Patients have less lag time between an identified need and the delivery of medication, which increases their sense of control and can decrease the amount of medication needed.
- Morphine (Roxanol, MS Contin), hydromorphone (Dilaudid), and fentanyl (Duragesic) are typical opioids for PCA delivery.
- Patients should be encouraged to inform their health care team if the PCA pump does not adequately control the pain.
- It is widely recommended that caregivers and family members be educated on the potential for inadvertent overdosing when the PCA button is pressed by anyone other than the patient, also called PCA by proxy.
- Clear institutional criteria regarding which patients should receive PCA and careful patient assessment throughout PCA use are essential to ensure safety (Berger & O’Neill, 2022).
Opioid Assessment
There are several tools available for assessing opioid risk. To balance pain management and safety when prescribing opioids, evidence-based guidelines recommend that clinicians who prescribe opioids use risk assessment instruments in patients before starting opioid therapy. The most common tools used include:
- Opioid Risk Tool (ORT): brief self-administered form with 10 yes or no questions about history of SUD, age, history of sexual abuse, and history of psychologic disease
- Screener and Opioid Assessment for Patients with Pain (SOAPP): 14-item self-administered form that asks about mood, smoking, family history, AA meeting attendance, prescription misuse, cravings, illegal drug use, and legal history
- Screener and Opioid Assessment for Patients with Pain-Revised (SOAPP-R): a revised version of the above with an additional 10 items, including home tension, sexual abuse history, and temper
Additionally, the Prescription Drug Monitoring Program (PDMP) should be reviewed prior to prescribing any controlled substance and periodically during treatment. Urine drug monitoring should also be implemented. Prior to administration, all patients should sign a controlled substance agreement, which includes safe storage and safe disposal of opioids (Manchikanti et al., 2023; Rosenquiest, 2025).
Stepwise Approach to Opioid Use
Best practice guidelines recommend that HCPs maximize nonopioid pharmacologic and nonpharmacologic therapies as appropriate for the specific condition before prescribing opioids. The American Society of Interventional Pain Physicians (ASIPP) last updated its opioid use for chronic noncancer pain guidelines in 2023. As noted in the guidelines, the pharmacological treatment of chronic pain (excluding cancer patients and end-of-life care) should always begin with nonopioid treatment options, as above (Manchikanti et al., 2023). If opioids are appropriate, HCPs must ensure patients know the expected benefits and risks before starting treatment. When the severity of acute pain warrants the use of opioids, the updated 2022 CDC clinical practice guidelines suggest prescribing immediate-release (IR) opioids at the lowest effective dose and for no longer than the expected duration of pain severe enough to require opioids. HCPs should prescribe and advise opioid use only PRN instead of on a scheduled basis. The initial opioid prescription should be considered a trial, with a follow-up appointment scheduled at a predetermined time to review the effectiveness of treatment and reassess the continued need for opioids (Dowell et al., 2022; Manchikanti et al., 2023).
IR medications with a half-life of 2–4 hours should be started initially with opioid-naive patients until the dose is stabilized, and patients should never be started on LA opioids initially. Dose adjustments may be necessary as often as every 2–3 days. The dose should be slowly titrated with the goal of treatment to administer the lowest dose that relieves pain with the fewest adverse effects. Every opioid works a little differently; therefore, each must be titrated to meet the patient's needs while minimizing toxicity and harm from adverse effects. ER or LA formulations with a half-life of 8–12 hours in the same family are commonly added later if long-term use is required and once the dose has been established. The meaningful benefits of opioids should continue to be addressed. Those patients who do not have pain relief from opioids within a month's time frame are unlikely to benefit in 6 months. A follow-up appointment within 1–4 weeks of starting opioids or dose increases is recommended to assess benefits and any harms. Once stable, all patients should be seen at least every 8–12 weeks with periodic drug screens and prescription drug monitoring program review. Those in the moderate- or high-risk categories should be seen more frequently and have clinical visits for refills (Dowell et al., 2022; Manchikanti et al., 2023; Rosenquist, 2025).
Assessing the patient’s pain level, functional abilities, and quality of life at each visit will indicate whether the current treatment plan is performing successfully. If, at any point, the risks outweigh the benefits, opioids should be tapered to a lower dose or gradually discontinued and other treatments optimized. Providers should reassess the risks and benefits of treatment when prescribing more than 50 MME per day and avoid (and carefully justify) prescribing more than 90 MME per day. According to the CDC’s Guideline for Prescribing Opioids for Pain, the risk of overdose is increased by at least twice in patients taking 50 MME per day or more, as compared to patients taking less than 20 MME per day; 50 MME is about 50 mg of hydrocodone or 33 mg of oxycodone daily. Prescribers should become familiar with and maintain access to a current MME calculator for dosage changes and transitions between medications to establish equivalent dosages. Several dose calculators are available online, including on the CDC and Centers for Medicare & Medicaid Services websites. However, these calculators have limitations and complicated exceptions (Dowell et al., 2022; Manchikanti et al., 2023; Rosenquist, 2025).
CDC 2022 Clinical Practice Guideline for Prescribing Opioids for Pain
The CDC encourages the appropriate treatment of pain, carefully considering the benefits and risks of all treatment options in the context of the patient’s circumstances. The CDC's Clinical Practice Guideline for Prescribing Opioids for Pain was updated in 2022 and replaced the 2016 version, which was limited to prescribing opioids for chronic pain only. The updated guideline now includes recommendations for HCPs when initiating or continuing opioid use for acute, subacute, and chronic pain. The guideline is a clinical tool intended to improve communication between HCPs and patients about the benefits and risks of pain treatments, including opioid therapy, to improve the effectiveness and safety of pain treatment, mitigate pain, improve function and quality of life for patients, and reduce the risks associated with opioid use, including OUD, overdose, and death. The guideline addresses the following four major areas:
- determining whether (or not) to initiate opioids for pain
- selecting opioids and determining opioid dosages
- deciding the duration of the initial opioid prescription and conducting follow-up
- assessing risk and addressing potential harms of opioid use (Dowell et al., 2022)
CDC’s Recommendations for Prescribing Opioids for Outpatients
The guideline includes 12 recommendations for HCPs prescribing opioids for outpatients. Table 7 outlines each recommendation as adapted directly from the guideline. It is important to note that these recommendations do not apply to pain related to sickle cell disease, cancer, or to patients receiving palliative or end-of-life care (CDC, 2024a; Dowell et al., 2022).
Table 7
CDC Recommendations for Prescribing Opioids for Outpatients
Determining Whether or Not to Initiate Opioids for Pain “All patients with pain should receive treatment that provides the greatest benefits relative to risks. Recommendations 1 and 2 address determining whether to initiate opioids for pain.
Recommendation 1
Recommendation 2
|
Selecting Opioids and Determining Opioid Dosages
Recommendation 4
Recommendation 5
|
Deciding Duration of Initial Opioid Prescription and Conducting Follow-Up Recommendations 6 and 7 address the duration of opioid therapy and routine patient follow-up. Recommendation 6
Recommendation 7
|
Assessing Risk and Addressing Potential Harms of Opioid Use Assessing risk and addressing potential harms of opioid use are addressed by recommendations 8 through 12. Recommendation 8
Recommendation 9
Recommendation 10
Recommendation 11
Recommendation 12
|
(CDC, 2024a; Dowell et al., 2022)
In addition, the following five guiding principles are endorsed to broadly inform implementation across the recommendations (Dowell et al., 2022):
- “Acute, subacute, and chronic pain need to be appropriately assessed and treated independent of whether opioids are part of a treatment regimen.
- Recommendations are voluntary and are intended to support, not supplant, individualized, person-centered care. Flexibility to meet the care needs and the clinical circumstance of a specific patient is paramount.
- A multimodal and multidisciplinary approach to pain management, attending to the physical health, behavioral health, long-term services and supports, and expected health outcomes and well-being of each person, is critical.
- Special attention should be given to avoid misapplying this clinical practice guideline beyond its intended use or implementing policies purportedly derived from it that might lead to unintended and potentially harmful consequences for patients.
- Clinicians, practices, health systems, and payers should vigilantly attend to health inequities; provide culturally and linguistically appropriate communication, including communication that is accessible to persons with disabilities; and ensure access to an appropriate, affordable, diversified, coordinated, and effective nonpharmacologic and pharmacologic pain management regimen for all persons” (Dowell et al., 2022).
Opioid Use in Special Populations
Special considerations should be applied when prescribing opioids to populations at potentially higher risk for harm, such as older adults (over 65 years), those with renal or hepatic insufficiency, and those who are pregnant. Advancing age is often accompanied by physiological changes that affect medication absorption, metabolism, and excretion. Older adults are also at increased risk for falls and fractures related to opioids. Prescribers should consider the risk of falls when selecting and dosing potentially sedating medications such as TCAs, antidepressants, and opioids. When less harmful alternative pharmacological modalities are ineffective, prescribers are encouraged to initiate therapy with these substances at the lowest possible dose and gradually increase as needed (i.e., “start low and go slow”). When prescribing opioids to older adults, an appropriate bowel regimen should be initiated to prevent constipation (Dowell et al., 2022). According to the BC, opioids should be avoided in older adults except in cases of severe, acute pain. It was also added to the list of drugs that may exacerbate delirium, and additional notations were added regarding the serious risk of sedation related to concomitant use of opioids and benzodiazepines (2023 AGS Beers Criteria Update Expert Panel, 2023).
Though opioid use in pregnancy is not well studied, it has known risks to the female parent and the fetus (Dowell et al., 2022). In 2014, the FDA removed the older system of ranking medications for pregnant patients (Category A, B, C, D, and X) and now requires detailed, specific information about pregnancy safety (including during labor and delivery), safety while breastfeeding, and safety for females and males of reproductive potential (FDA, 2025). Some studies have shown an association between opioid use during pregnancy and congenital disabilities, including neural tube defects, congenital heart defects, preterm delivery, poor fetal growth, stillbirth, and potential for neonatal opioid withdrawal syndrome (Dowell et al., 2022). Opioids are excreted in breast milk and increase the risk for CNS and respiratory depression in the infant if taken by the female parent while breastfeeding. These risks can be minimized using the lowest effective dose to control pain. Prescribers must inform patients of the potential risks before prescribing opioids and other controlled substances. Acetaminophen (Tylenol) is generally considered safe during pregnancy and while breastfeeding. The FDA (2020) issued a safety communication advising females to avoid using NSAIDs in pregnancy at 20 weeks or later due to the risk of bleeding, premature ductal closure, and rare but serious kidney problems in the unborn baby. There is limited data on the safe use of NSAIDs while breastfeeding, and the FDA advises breastfeeding patients to consult with their health care professionals before taking these medications (FDA, 2020).
Cancer Patients and Pain Management at the End-of-Life
The treatment of cancer pain is highly complex, and the patient's disease prognosis, concurrent medications, and individual goals of care should be carefully considered for all decision-making (Portenoy et al., 2026). Pain treatment within the specialty care of terminally ill patients does not typically conform to the standard regulations. There is less concern for misuse, abuse, or addiction, and emphasis should be on ensuring effective pain relief (Dowell et al., 2022). However, fears continue to focus on overdose, respiratory depression, and potential loss of consciousness or hastening of the end-of-life. According to the National Coalition for Hospice and Palliative Care (NCHPC) Clinical Practice Guidelines for Quality Palliative Care, analgesics should be increased gradually and as tolerated, with the patient's full consent or their health care proxy (or via their living will or advance directives). The patient and/or caregivers should be fully informed of the potential risks of increased opioid doses. If the patient and family prioritize pain relief over the length of life, the care team should accept and respect that decision. It is generally accepted that clinicians should never withhold needed pain medication from terminally ill patients for fear of hastening death if they have received informed consent from the patient to do so. Loss of consciousness should not always be assumed to be directly caused by high doses of opioid painkillers in the dying patient if those doses have been stable or slowly increasing, especially in chronic cancer pain (NCHPC, 2018).
Complications of Opioid Use
There are several adverse effects associated with opioid use, which vary in severity based on the dose and potency of the medication, administration route, and whether the drug is self-administered or administered by a nurse or other caregiver. The most common side effects of opioids include orthostatic hypotension, urinary retention, nausea, and constipation. Patients should be advised to sit or lie down if experiencing orthostatic hypotension (e.g., lightheadedness or dizziness) and avoid sudden changes in positioning (e.g., moving slowly from lying to sitting or standing). To manage urinary retention, monitor intake/output, assess for bladder distention, administer bethanechol (Urecholine), and exhaust all noninvasive actions before catheterizing. Nausea and vomiting can be managed with antiemetic medications, oral hydration, dietary modifications, and elimination of offending odors. A preventative approach to constipation should be implemented with each patient receiving opioids. Strategies include monitoring bowel movements, increasing fluids, adding dietary fiber, increasing hydration, and engaging in daily exercise. In addition, patients should be given stool softeners, stimulant laxatives, and/or enemas as clinically indicated (Berger & O’Neill, 2022; Rosenquist, 2025).
The most severe complication of opioid use is overdose. Signs and symptoms of opioid toxicity and overdose include respiratory depression, coma, and pinpoint pupils (also referred to as the opioid triad). Sedation always precedes respiratory depression, so the patient's level of consciousness should be monitored closely so steps can be promptly taken to reduce the dose or administer a reversal agent if required. The initial treatment of respiratory depression and sedation is generally a reduction in the opioid dose, carefully titrating the dose while closely monitoring the patient’s respiratory status. When an overdose is suspected, naloxone (Narcan) should be administered to reverse the opioid effects until the patient can breathe deeply with a respiratory rate of at least 8/minute. Most patients respond to naloxone (Narcan) by returning to spontaneous breathing within 2–3 minutes of administration. However, some patients may require ventilatory support, rescue breathing, and chest compressions while awaiting the return of spontaneous breathing. All patients should be monitored for at least 4 hours after the last dose of naloxone (Narcan) for signs of recurrence of opioid toxicity. Patients who overdose on LA opioids may require prolonged monitoring. Finally, opioid withdrawal triggered by naloxone (Narcan) causes several distressing symptoms in patients physically dependent on these agents. The most common signs and symptoms include agitation, irritability, tachycardia, fever, nausea, vomiting, diarrhea, rhinitis, diaphoresis, nervousness, restlessness, weakness, insomnia, and increased blood pressure (Berger & O’Neill, 2022; Stolbach & Hoffman, 2026).
Opioid Abuse and Misuse
The number of opioid-related deaths increased significantly from 1999 to 2023, and 2023 was the first decline seen since 2018. The three waves of increase over these years have been driven by a different type of opioid. The first wave involved prescription opioids, the second wave involved heroin, and the third wave involved synthetic opioids (illegal fentanyl and fentanyl analogs). In 2023, drug overdoses resulted in 105,000 deaths, with 76% of these involving opioids. This is about 217 people per day, which is 10 times the number of overdose deaths in 1999. From 2022 to 2023, the rate of overdose deaths by synthetic opioids decreased by 2%, heroin decreased by 33%, and prescription opioids decreased by 12%. The CDC continues to monitor trends, advance research, HCPs, and systems, partnering with public safety officials, and increasing public awareness to confront the opioid overdose epidemic (CDC, 2025c). In 2024, 2.1 million people in the United States, 12 years and older, reported misusing prescription pain relievers. Of these, 43.7% reported getting or stealing the prescription from an HCP, 42.3% reported getting it from a friend or relative, and 7.6% reported buying it from a drug dealer or stranger. Of the medications, hydrocodone was the most abused in 2024, followed by oxycodone, codeine, tramadol, buprenorphine, fentanyl, morphine, methadone, hydromorphone, oxymorphone, and Demerol, in that order (SAMHSA, 2025).
Contributing and Risk Factors for Potential Misuse/Abuse
The progressive rise in prescription drug misuse/abuse across the United States is a byproduct of the complex interplay of many contributing factors. However, the prescribing of opioid analgesics is a preeminent contributing factor in drug availability and, in turn, misuse/abuse potential. Additional societal and environmental factors include aggressive marketing by the pharmaceutical industry, the explosion of illegal web-based pharmacies that dispense these medications without proper prescriptions and surveillance, and greater social acceptability for medicating a growing number of conditions (HHS, 2019). Personal risk factors for potential drug misuse/abuse include co-occurring mental health disorders, younger age, past or current SUD (including alcohol and tobacco use), family history of SUD, and history of childhood mistreatment. The prevalence of OUD at the time of delivery has also increased, which is concerning for increased rates of neonatal abstinence syndrome. The health consequences of OUD can be debilitating. These include the more obvious consequences of overdose and death, as well as less obvious consequences such as infection from contaminated drugs or equipment, increased risk of cancer, and motor vehicle-related injuries. Systemic effects on the body include opioid-induced bowel syndrome, opioid-induced hyperalgesia, opioid-associated liver fibrosis, opioid-related leukoencephalopathy, and opioid amnestic syndrome (Strain, 2024).
Opioid Use Disorder
OUD is defined in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition Text Revision (DSM-5-TR) as a destructive repetition or habit of ingesting or administering opioids that causes the following substantial anguish or drastically affects the patient’s ability to function professionally, socially, or otherwise, as evidenced by two or more of the conditions listed here within 1 year:
- ineffective attempts to reduce the use of opioids or a wish to do so
- an intense need or impulse to ingest or administer opioids
- persistent ingestion of opioids even though they have experienced repeated relational challenges (i.e., with surrounding friends and family members) related to their use
- persistent ingestion of opioids in environments where it is unsafe
- the development of tolerance, which is a gradual reduction in the physical impact/effect of the opioids when administered at a consistent amount, requiring an increase in the amount to achieve the prior effect
- persistent ingestion of opioids for a longer time and at a higher amount than planned
- a considerable investment of time related to opioids, procuring them, ingesting them, or recuperating from the consequences of their use.
- persistent ingestion of opioids, leading to interference with significant responsibilities and commitments (i.e., academic, professional, or familial)
- a decrease in attendance or participation in significant events at work, at home, or with friends/family due to the use of opioids
- persistent ingestion of opioids even though they are aware of a significant challenge directly related to opioid use
- the development of withdrawal as evidenced by the signs and symptoms of opioid withdrawal syndrome or the use of opioids to prevent these symptoms (American Psychiatric Association [APA], 2022, pp. 608–609)
This diagnosis may be graded as mild (two or three symptoms), moderate (four or five), or severe (at least six symptoms). The diagnosis may be considered in early (3 or more months) or sustained (12 or more months) remission when all the above symptoms have resolved, except for an intense need or impulse to use the substance. This diagnosis may also be qualified in a controlled environment if the patient lacks substance access.
This diagnosis may also be qualified as on maintenance therapy if the patient is currently on a prescribed opioid agonist (e.g., buprenorphine or methadone; APA, 2022, pp. 608–609).
The Safe and Effective Prescribing of Opioids
Opioids and all other types of controlled substances are classified according to categories or "schedules" based on the perceived risk of addiction as outlined by the Drug Enforcement Administration (DEA). Schedule 1 drugs, substances, and chemicals are not acceptable for medical use and have the highest potential for abuse. Examples of these include heroin and marijuana. Schedule 2 drugs, substances, and chemicals have a high potential for abuse and dependence. Examples include methadone (Dolophine), hydromorphone (Dilaudid), and oxycodone (OxyContin). Schedule III drugs, substances, and chemicals have moderate to low abuse and dependence potential. These include Tylenol with codeine (Tylenol #3) and ketamine (Ketalar). Schedule IV drugs, substances, and chemicals have low potential for abuse and dependence. These include tramadol (Ultram) and carisoprodol (Soma). Schedule V drugs, substances, and chemicals have the lowest potential for abuse and include codeine/guaifenesin (Robitussin AC) and pregabalin (Lyrica; DEA, n.d.). State laws, regulations, and policies further delineate prescriber responsibilities surrounding prescribing and dispensing controlled substances. The HHS increased grant funding toward developing novel strategies to impede this growing and deadly problem. These efforts have brought a higher level of urgency to the matter, with heightened surveillance, restriction, and monitoring of patients on long-term opioid therapy. All prescribers must be registered with the DEA and be granted prescriptive authority. Prescribers must also understand the legislative details and state mandates for prescribing and monitoring opioids. It is equally imperative for health care professionals to remain vigilant in screening for the signs and symptoms of misuse and abuse. New requirements in 2023 also require all providers registering for a new or updated DEA license to take 8 hours of training on OUDs or SUDs unless they are board-certified in addiction or graduated and took an opioid course within 5 years (SAMHSA, 2024).
As part of the national movement to mitigate the opioid epidemic, all 50 states and the District of Columbia have implemented statewide electronic databases, PDMPs, to track and monitor opioid prescriptions (American Association of Nurse Practitioners [AANP], 2025). A PDMP is a statewide electronic database that collects data on controlled substances dispensed to or for each patient. The intent is to improve opioid prescribing, inform clinical practice, and protect high-risk patients. Prescribers and dispensers are subject to state-specific reporting requirements, which may vary by state. PDMPs are housed and operated by state regulatory, administrative, or law enforcement agencies. The housing agency disseminates information from the database to individuals authorized under state law to receive the information for purposes identified by the state. States arrange individual systems to track and monitor prescriptions. The details about use, access, and which drugs are included, and the regulations and implications for prescribers vary significantly by state. Most states have a method by which prescribers can access their patient's records in other or neighboring states besides their own. The key to the efficacy of PDMP systems is the mandate that all prescribers or an appropriate delegate (e.g., nurse) check the system before initiating opioid therapy. Reviewing the patient's history of controlled substance prescriptions using the PDMP database helps to determine whether the patient is already receiving opioids or potentially dangerous combinations that place them at risk for overdose. Differences exist between the states regarding how frequently providers should monitor this system and which controlled substances are included. Reporting systems help reduce the diversion of illegitimate opiate prescriptions (AANP, 2025; CDC, 2024c).
Once opioid therapy is initiated, prescribers are responsible for assessing and monitoring potential signs of opioid misuse throughout treatment. Several risk assessment instruments are available to assist prescribers with ongoing monitoring. Some of the most commonly used tools include the following:
- Diagnosis, Intractability, Risk, Efficacy (DIRE)
- Opioid Risk Tool-Opioid Use Disorder (ORT-OUD)
- Current Opioid Misuse Measure (COMM)
- Addiction Behavior Checklist (ABC; Rosenquist, 2025)
In addition to using PDMPs and monitoring instruments, other risk mitigation strategies include having patients return for more frequent monitoring intervals and performing random pill counts. Some states require HCPs to monitor for signs of abuse, misuse, or diversion by performing unannounced urine drug testing (UDT) throughout the year (Rosenquist, 2025). The CDC (Dowell et al., 2022) recommends that UDTs be performed before starting opioid therapy and at least once annually to assess for prescribed medications, other controlled prescription drugs, and illicit drugs.
Patient–Provider Agreements and Opioid Contracts
Although there is little efficacy regarding opioid agreements, some states have laws mandating patient–provider agreements (PPA) or opioid contracts. PPAs are written agreements between prescribers and patients outlining and clarifying the conditions for prescribing opioids over the long term, and they can help formalize safer approaches to opioid prescribing (Rosenquiest, 2025). The CDC (Dowell et al., 2022) recommends a flexible agreement rather than a punitive contract. The agreement underscores the critical importance of properly taking pain medications, outlining the standards of care and treatment expectations. It promotes collaboration and mutual commitment from both parties, sets realistic expectations with measurable goals for therapy, and states reasons for which the agreement may be terminated. In addition, these agreements should address the potential adverse effects, possible overdose, respiratory depression, development of physical dependence or tolerance, drug interactions, inadvertent ingestion by children or others, and drug misuse or abuse by the patient, as well as household contacts or friends. Furthermore, prescribing policies should be clearly defined, including the number and frequency of refills, policy on early refills, and procedures for lost, damaged, or stolen medications. If UDTs or pill counts are to be performed periodically, this should be included in the agreement, along with how medication refills and changes should be requested and obtained by the patient and handled by the office staff and providers (Rosenquist, 2025). A sample opioid PPA is available through the FDA (FDA, n.d.).
Documentation
Documentation is critical when prescribing and monitoring patients taking controlled substances, both for safety and legal reasons. Documentation in the medical record should be clear, concise, and include all details outlining dose adjustments or medication changes with associated justifications and equivalency calculations. Documentation should also include the effectiveness of treatments based on consistent pain and other assessments repeated at each visit, as well as any adverse effects and related therapies. Documentation should also specify if the patient is adhering to treatment plans as outlined in the PPA and include the results of UDTs or pill counts. Any concerning or aberrant behavior should be carefully documented with as much detail as possible. Interviews with family members and caregivers can also be included in documentation records for those same reasons, with a clear plan for resolution and/or future monitoring. Any letters sent to patients should be included in the patient's medical record, and office staff should carefully document any phone calls made or received. Document every time PDMP reports are reviewed and any concerning findings. A decision to terminate care needs to be documented thoroughly (Dowell et al., 2022; Federation of State Medical Boards [FSMB], 2024; Rosenquist, 2025).
Termination of Chronic Opioid Therapy
Treating any medical condition aims to restore health and resume pre-illness ADLs; the same is true for terminating chronic opioid therapy. Opioid therapy may be stopped or tapered for various reasons, such as the healing of the initial pain-causing condition, the appearance of unbearable side effects, insufficient pain relief, lack of enhancement in the patient's quality of life despite proper dosage adjustments, failure to attain anticipated pain alleviation or functional progress, patient's request, major nonadherence with the treatment plan, development of SUD, or notable misuse of medication. Furthermore, HCPs should only maintain opioid treatment if the patient has experienced benefits like improved functionality, enhanced quality of life, or at least a slowdown in their deterioration (FSMB, 2024; Pisansky et al., 2026).
Appropriate termination helps to avoid a perceived betrayal of trust or abuse of power, prevents harm, and conveys caring. The PPA plays a critical role in this process; therefore, termination must be addressed comprehensively in the initial contractual agreement and updated accordingly. Termination always carries considerable risks, including exposing the patient to severe pain, withdrawal symptoms, mental health crises, illicit opioid use, and suicide. Unless the patient is in a life-threatening situation, opioids should not be abruptly discontinued. When considering a tapering approach, the objective should not necessarily be to completely stop opioid use but to determine the appropriate dosage that maximizes benefits while minimizing risks. APRNs should carefully evaluate the pros and cons of continuing versus tapering opioids in partnership with the patient. Prior to stopping or tapering opioids, it is important to evaluate the patient for factors that might hinder the success of the taper or elevate the risks noted above. These factors include OUD, mental health conditions (i.e., anxiety and depression), psychological rigidity, high levels of reported pain, and the use of opioids as a means of self-medicating for functional purposes. If opioids are to be discontinued, patients who have developed physical dependence should be given a carefully structured tapering plan. This plan should be developed collaboratively with the patient, including decisions on the pace of tapering and when to pause the process if needed. APRNs should reassure patients that this change does not indicate the end of their treatment, which can proceed with other modalities or through another HCP if necessary. Since discontinuing opioids can be challenging for some patients, a referral to an addiction specialist may be required for those on very high doses of opioids. APRNs are responsible for ensuring a smooth transition to minimize negative outcomes (FSMB, 2024; Pisansky et al., 2026).
Strategies for termination of chronic opioid therapy include the following:
- Establish open, honest communication and dialogue with the patient from the point of the initial consultation.
- Comprehensively address termination in the informed consent and PPA process and readdress or refer to it as necessary during therapy.
- Set realistic, time-sensitive goals at the beginning of treatment.
- Balance clinical judgment and individualization; incidents or events that cause concern regarding a pain agreement need to be interpreted within the context of the whole patient.
- Opioid tapers should be performed after a discussion with the patient. There is no “one way” to taper a patient. Generally, the longer the patient has been on opioids, the longer it will take for a successful taper.
- Avoid terminating the relationship when a patient is in crisis without referral to a specialized facility and a warm handoff to the receiving provider. If a patient is terminated while in crisis, it might be considered abandonment and escalate abhorrent behaviors.
- As part of the termination preparation process, the patient should be given information about other available resources (e.g., community resources, support groups, and nonpharmacological pain modalities). The HCP should document the resources provided (Dowell et al., 2022; FSMB, 2024; Pisansky et al., 2026).
The evidence on how to taper long-term opioid users with chronic noncancer pain is not robust. Those taking more than 50 mg morphine equivalents per day have a higher risk of mortality when stopping opioids; however, this is not a strict limit for the need to taper. For patients who have been on opioids for more than 1 year, it is recommended to taper by 10% each month. Withdrawal symptoms can be managed with a2-adrenergic agonists such as clonidine (Catapres), lofexidine (Lucemyra), or tizanidine (Zanaflex). Tizanidine (Zanaflex) is often a first-line agent for myalgias and sympathetic symptoms. It is dosed at 2–4 mg every 6–8 hours as needed (Pisansky et al., 2026).
The APRN’s Role in Ensuring Adequate Pain Management
The APRN should take a proactive approach by frequently assessing and reassessing patients for pain. Ensuring analgesics are prescribed and given before pain becomes too severe promotes adequate pain control. The APRN should instruct hospitalized patients to report developing or recurrent pain early and not wait until the pain is severe to ask for their as-needed pain medications. It takes less medication to prevent pain than to treat pain. The APRN should explain misconceptions and myths about pain to reduce the patient’s fear and anxiety regarding pain medication. This education can help promote acceptance and compliance by patients reluctant to take opioids due to addiction-related concerns. For chronic and uncontrolled pain patients, administer analgesics consistently rather than PRN by prescribing an LA or ER opioid analgesic (including the transdermal route; Dowell et al., 2022).
Providing adequate pain management without promoting OUD is complicated and challenging for HCPs. Concerns about OUD should not be minimized. To address the current epidemic of OUD in the United States., the FDA has already taken steps to reduce public exposure, prevent OUD, and support those with the disorder. Recently, it has launched an innovative challenge to further combat the opioid crisis by encouraging the development of medical devices. The FDA is working with the medical device companies as they submit FDA applications and expedited reviews, ensuring safety and effectiveness. These devices include:
- Rapid drug screen
- Brainway Deep Transcranial Magnetic Stimulation Device
- Virtual Reality Neuropsychological Therapy
- IPill Dispenser
- SafetyNet Opioid System
- Opioid Prediction Service
- NanoThermTM and VascuThermTM Systems (FDA, 2024)
References
American Association of Nurse Practitioners. (2025). Issues at a glance: Prescription drug monitoring programs (PDMPs). https://www.aanp.org/advocacy/advocacy-resource/policy-briefs/issues-at-a-glance-prescription-drug-monitoring-programs-pdmp
American Geriatrics Society Beers Criteria Update Expert Panel. (2023). American Geriatrics Society 2023 updated AGS Beers Criteria® for potentially inappropriate medication use in older adults. Journal of the American Geriatrics Society, 71(7), 2052–2081. https://doi.org/10.1111/jgs.18372
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders: Text revision, DSM-5-TR (5th ed.). Author.
Arcangelo, V. P., Peterson, A. M., Wilbur, V. F., & Kang, T. M. (2022). Pharmacotherapeutics for advanced practice (5th ed.). Wolters Kluwer.
Barad, M., & Aggarwal, A. (2026). Overview of pain. Merck Manual Professional Version. Retrieved March 16, 2026, from https://www.merckmanuals.com/professional/neurologic-disorders/pain/overview-of-pain
Barnett, A. K., & Boyer, E. W. (2025). Salicylate (aspirin) poisoning: Clinical manifestations and evaluation. UpToDate. Retrieved March 18, 2026, from https://www.uptodate.com/contents/salicylate-aspirin-poisoning-clinical-manifestations-and-evaluation
Berger, A. M., & O’Neill, J. F. (2022). Principles and practices of palliative care and supportive oncology (5th ed.). Wolters Kluwer.
Bickley, L. S., Szilagyi, P. G., Hoffman, R. M., & Soriano, R. P. (2020). Bates’ guide to physical examination and history taking (13th ed.). Wolters Kluwer.
Burns, M. J., Friedman, S. L., & Larson, A. M. (2024). Acetaminophen (paracetamol) poisoning in adults: Pathophysiology, presentation, and evaluation. UpToDate. Retrieved March 18, 2026, from https://www.uptodate.com/contents/acetaminophen-paracetamol-poisoning-in-adults-pathophysiology-presentation-and-evaluation
Camacho, P. M., Petak, S. M., Binkley, N., Diab, D. L., Eldeiry, L. S., Farooki, A., Harris, S. T., Hurley, D. L., Kelly, J., Lewiecki, E. M., Pessah-Pollack, R., McClung, M., Wimalawansa, S. J., & Watts, N. B. (2020). American Association of Clinical Endocrinologists/American College of Endocrinology clinical practice guidelines for the diagnosis and treatment of postmenopausal osteoporosis—2020 update executive summary. Endocrine Practice, 26(5), 564–570. https://doi.org/10.4158/GL-2020-0524
Cao, B., Xu, Q., Shi, Y., Zhao, R., Li, H., Zheng, J., Liu, F., Wan, Y., & Wei, B. (2024). Pathology of pain and its implications for therapeutic interventions. Signal Transduction and Targeted Therapy, 9, 155. https://doi.org/10.1038/s41392-024-01845-w
Centers for Disease Control and Prevention. (2024a). Guideline recommendations and guiding principles: 2022 clinical practice guideline recommendations. https://www.cdc.gov/overdose-prevention/hcp/clinical-guidance/recommendations-and-principles.html
Centers for Disease Control and Prevention. (2024b). Overdose prevention: Commonly used terms. Retrieved March 26, 2026, from https://www.cdc.gov/overdose-prevention/glossary/
Centers for Disease Control and Prevention. (2024c). Prescription drug monitoring programs (PDMPs). Retrieved March 26, 2026, from https://www.cdc.gov/overdose-prevention/php/interventions/prescription-drug-monitoring-programs.html
Centers for Disease Control and Prevention. (2025a). About shingles (Herpes Zoster). Retrieved March 26, 2026, from https://www.cdc.gov/shingles/about/
Centers for Disease Control and Prevention. (2025b). Lifesaving naloxone. Retrieved March 26, 2026, from https://www.cdc.gov/stop-overdose/caring/naloxone.html
Centers for Disease Control and Prevention. (2025c). Understanding the opioid overdose epidemic. Retrieved March 26, 2026, from https://www.cdc.gov/overdose-prevention/about/understanding-the-opioid-overdose-epidemic.html
Chiriboga, C. A. (2025). Acute toxic-metabolic encephalopathy in children. UpToDate. Retrieved March 18, 2026, from https://www.uptodate.com/contents/acute-toxic-metabolic-encephalopathy-in-children
Chou, R. (2026). Subacute and chronic low back pain: Management. UpToDate. Retrieved April 25, 2023, from https://www.uptodate.com/contents/subacute-and-chronic-low-back-pain-nonpharmacologic-and-pharmacologic-treatment
Coffin, P. (2026). Prevention of lethal opioid overdose in the community. UpToDate. Retrieved March 19, 2026, from https://www.uptodate.com/contents/prevention-of-lethal-opioid-overdose-in-the-community
Copenhaver, D. J., Pritzlaff, S. G., Jung, M., & Singh, N. S. (2025). Interventional therapies for chronic pain. UpToDate. Retrieved March 16, 2026, from https://www.uptodate.com/contents/interventional-therapies-for-chronic-pain
Dowell, D., Ragan, K. R., Jones, C. M., Baldwin, G. T., & Chou, R. (2022). CDC clinical practice guideline for prescribing opioids for pain—United States, 2022. Morbidity and Mortality Weekly Report (MMWR), 71(3), 1–95. https://doi.org/10.15585/mmwr.rr7103a1
Federation of State Medical Boards. (2024). Strategies for prescribing opioids for the management of pain. https://www.fsmb.org/siteassets/advocacy/policies/strategies-for-prescribing-opioids-for-the-management-of-pain.pdf
Feldman, E. L. (2025). Epidemiology and classification of diabetic neuropathy. UpToDate. Retrieved March 20, 2026, from https://www.uptodate.com/contents/epidemiology-and-classification-of-diabetic-neuropathy
Goldenberg, D. L., & Kaplan, M. (2025a). Fibromyalgia: Clinical manifestations and diagnosis in adults. UpToDate. Retrieved March 20, 2026, from https://www.uptodate.com/contents/fibromyalgia-clinical-manifestations-and-diagnosis-in-adults
Goldenberg, D. L., & Kaplan, M. (2025b). Fibromyalgia: Treatment in adults. UpToDate. Retrieved March 20, 2026, from https://www.uptodate.com/contents/fibromyalgia-treatment-in-adults
Heard, K., & Dart, R. (2025). Acetaminophen (paracetamol) poisoning: Management in adults and children. UpToDate. Retrieved March 18, 2026, from https://www.uptodate.com/contents/acetaminophen-paracetamol-poisoning-in-adults-treatment
Ho, C. C., Khan, S. A., & Whealy, M. A. (2026). Trigeminal neuralgia. UpToDate. Retrieved March 18, 2026, from https://www.uptodate.com/contents/trigeminal-neuralgia
Hosseini, F., Mullins, S., Gibson, W., & Thake, M. (2022). Acute pain management for older adults. Clinical Medicine Journal, 22(4), 302–306. https://doi.org/10.7861/clinmed.22.4.ac-p
Ignatavicius, D. D., Rebar, C. R., & Heimgartner, N. M. (2024). Medical-surgical nursing: Concepts for clinical judgement and collaborative care (11th ed.). Elsevier.
International Association for the Study of Pain. (2021). Terminology. Retrieved March 16, 2026, from https://www.iasp-pain.org/resources/terminology/?navItemNumber=576#Pain
Kalapatapu, V. (2025). Lower extremity amputation. UpToDate. Retrieved March 20, 2026, from https://www.uptodate.com/contents/lower-extremity-amputation
Kissoon, N. R. (2026). Postherpetic neuralgia. UpToDate. Retrieved March 20, 2026, from https://www.uptodate.com/contents/postherpetic-neuralgia
Knight, C. L., & Chou, R. (2026). Treatment of acute low back pain. UpToDate. Retrieved March 19, 2026, from https://www.uptodate.com/contents/treatment-of-acute-low-back-pain
Lucas, J. W., & Sohi, I. (2024). Chronic pain and high-impact chronic pain in U.S. Adults, 2023. National Center for Health Statistics. https://www.cdc.gov/nchs/products/databriefs/db518.htm
Mallick-Searle, T., & Adler, J. A. (2024). Update on treating painful diabetic peripheral neuropathy: A review of current US guidelines with a focus on the most recently approved management options. Journal of Pain Research, 17, 1005–1028. https://doi.org/10.2147/JPR.S442595
Manchikanti, L., Kaye, A. M., Knezevic, N. M., Giordano, J., Applewhite, M. K., Bautista, A., Soin, A., Blank., S. K., Sanapati, M. R., Karri, J., Christo, P. J., Abd-Elsayed, A., Kaye, A. D., Calodney, A., Navani, A., Gharibo, C. G., Harned, M., Gupta, M., Broachwala, M. … Hirsch, J. A. (2023). Comprehensive, evidence-based, consensus guidelines for prescription of opioids for chronic non-cancer pain from the American Society of Interventional Pain Physicians (ASIPP). Pain Physician, 26(7S), S7–S126. https://doi.org/10.36076/ppj.2023.26.S7
Mariano, E. R. (2026). Approach to the management of acute pain in adults. UpToDate. Retrieved March 16, 2026, from https://www.uptodate.com/contents/approach-to-the-management-of-acute-pain-in-adults
McCaffery, M. (1968). Nursing practice theories related to cognition, bodily pain, and man-environment interactions. University of California Print.
National Coalition for Hospice and Palliative Care. (2018). Clinical practice guidelines for quality palliative care (4th ed.). https://www.nationalcoalitionhpc.org/wp-content/uploads/2024/03/NCHPC67840.html
National Institute of Neurological Disorders and Stroke. (2026a). Pain. Retrieved March 16, 2026, from https://www.ninds.nih.gov/health-information/disorders/pain#3084_2
National Institute of Neurological Disorders and Stroke. (2026b). Trigeminal neuralgia. https://www.ninds.nih.gov/Disorders/All-Disorders/Trigeminal-Neuralgia-Information-Page
National Institute on Drug Abuse. (2021). Prescription opioids drugfacts. https://nida.nih.gov/publications/drugfacts/prescription-opioids
Pandharipande, P., & Hayhurst, C. J. (2025). Pain control in the critically ill adult patient. UpToDate. Retrieved March 18, 2026, from https://www.uptodate.com/contents/pain-control-in-the-critically-ill-adult-patient
Pisansky, A. J. B., Berna, C., & Rathmell, J. P. (2026). Opioid tapering for patients with chronic pain. UpToDate. Retrieved March 20, 2026, from https://www.uptodate.com/contents/opioid-tapering-for-patients-with-chronic-pain
Portenoy, R. K., Mehta, Z., & Ahmed, E. (2024). Prevention and management of side effects in patients receiving opioids for chronic pain. UpToDate. Retrieved March 19, 2026, from https://www.uptodate.com/contents/prevention-and-management-of-side-effects-in-patients-receiving-opioids-for-chronic-pain
Portenoy, R. K., Mehta, Z., & Ahmed, E. (2026). Cancer pain management with opioids: Optimizing analgesia. UpToDate. Retrieved March 19, 2026, from https://www.uptodate.com/contents/cancer-pain-management-with-opioids-optimizing-analgesia
Price, R., Smith, D., Franklin, G., Gronseth, G., Pignone, M., David, W. S., Armon, C., Perkins, B. A., Bril, V., Rae-Grant, A., Halperin, J., Licking, N., O’Brien, M. D., Wessels, S. R., MacGregor, L. C., Fink, K., Harkless, L. B., Colbert, L., & Callaghan, B. C. (2021). Oral and topical treatment of painful diabetic polyneuropathy: Practice guideline update summary. Neurology, 98(1), 31–43. https://doi.org/10.1212/WNL.0000000000013038
Rosenquist, R. (2025). Use of opioids in the management of chronic pain in adults. UpToDate. Retrieved March 19, 2026, from https://www.uptodate.com/contents/use-of-opioids-in-the-management-of-chronic-pain-in-adults
Schwenk, E. S. (2025). Nonopioid pharmacotherapy for acute pain in adults. UpToDate. Retrieved March 18, 2026, from https://www.uptodate.com/contents/nonopioid-pharmacotherapy-for-acute-pain-in-adults
Singh, D., & Saadabadi, A. (2023). Naltrexone. In StatPearls. StatPearls Publishing. Retrieved March 26, 2026, from https://www.ncbi.nlm.nih.gov/books/NBK534811/
Solomon, D. H. (2024). NSAIDs: Therapeutic use and variability of response in adults. UpToDate. Retrieved March 17, 2026, from https://www.uptodate.com/contents/nsaids-therapeutic-use-and-variability-of-response-in-adults
Solomon, D. H. (2025a). NSAIDs (including aspirin): Pharmacology and mechanism of action. UpToDate. Retrieved March 16, 2026, from https://www.uptodate.com/contents/nsaids-including-aspirin-pharmacology-and-mechanism-of-action
Solomon, D. H. (2025b). Overview of COX-2 selective NSAIDS. UpToDate. Retrieved March 17, 2026, from https://www.uptodate.com/contents/overview-of-cox-2-selective-nsaids
Solomon, D. H. (2026). Nonselective NSAIDs: Overview of adverse effects. UpToDate. Retrieved March 17, 2026, from https://www.uptodate.com/contents/nonselective-nsaids-overview-of-adverse-effects
Stolbach, A., & Hoffman, R. S. (2026). Acute opioid intoxication in adults. UpToDate. Retrieved March 19, 2026, from https://www.uptodate.com/contents/acute-opioid-intoxication-in-adults
Strain, E. (2024). Opioid use disorder: Epidemiology, clinical features, health consequences, screening, and assessment. UpToDate. Retrieved March 20, 2026, from https://www.uptodate.com/contents/opioid-use-disorder-epidemiology-clinical-features-health-consequences-screening-and-assessment
Strain, E. (2026). Opioid use disorder: Pharmacologic management. UpToDate. Retrieved March 19, 2026, from https://www.uptodate.com/contents/opioid-use-disorder-pharmacologic-management
Substance Abuse and Mental Health Services Administration. (2024). Waiver Elimination (MAT Act). Retrieved March 20, 2026, from https://www.samhsa.gov/substance-use/treatment/resources/mat-act
Substance Abuse and Mental Health Services Administration. (2025). Key substance use and mental health indicators in the United States: Results from the 2024 National Survey on Drug Use and Health (HHS Publication No. PEP25-07-007, NSDUH Series H-60). https://www.samhsa.gov/data/sites/default/files/reports/rpt56287/2024-nsduh-annual-national-report.pdf
Tauben, D., & Stacey, B. R. (2025). Overview of pharmacologic management of chronic pain in adults. UpToDate. Retrieved March 18, 2026, from https://www.uptodate.com/contents/overview-of-pharmacologic-management-of-chronic-pain-in-adults
Tauben, D., & Stacey, B. R. (2026a). Approach to the management of chronic non-cancer pain in adults. UpToDate. Retrieved March 16, 2026, from https://www.uptodate.com/contents/approach-to-the-management-of-chronic-non-cancer-pain-in-adults
Tauben, D., & Stacey, B. R. (2026b). Evaluation of chronic pain in adults. UpToDate. Retrieved March 16, 2026, from https://www.uptodate.com/contents/evaluation-of-chronic-pain-in-adults
Taylor, J. L., Regier, N. G., Li, Q., Liu, M., Szanton, S. L., & Skolasky, R. L. (2022). The impact of low back pain and vigorous activity on mental and physical health outcomes in older adults with arthritis. Frontiers in Pain Research (Lausanne), 3(886985), 1–10. https://doi.org/10.3389/fpain.2022.886985
Theriot, J., Sabir, S., & Azadfard, M. (2026). Opioid antagonists. In StatPearls. StatPearls Publishing. Retrieved March 26, 2026, from https://www.ncbi.nlm.nih.gov/books/NBK537079/
University of Florida Health. (n.d.). Pain assessment scales/tools. Retrieved March 16. 2026, from https://pami.emergency.med.jax.ufl.edu/resources/pain-assessment-scales/
UpToDate Lexidrug. (n.d.-a). Acetaminophen (paracetamol): Drug information. UpToDate. Retrieved March 18, 2026, from https://www.uptodate.com/contents/acetaminophen-paracetamol-drug-information
UpToDate Lexidrug. (n.d.-b). Duloxetine: Drug information. UpToDate. Retrieved March 19, 2026, from https://www.uptodate.com/contents/duloxetine-drug-information
UpToDate Lexidrug. (n.d.-c). Milnacipran: Drug information. UpToDate. Retrieved March 19, 2026, from https://www.uptodate.com/contents/milnacipran-drug-information
U.S. Department of Health and Human Services. (2019). Pain management best practices inter-agency task force report. Retrieved from https://www.hhs.gov/sites/default/files/pmtf-final-report-2019-05-23.pdf
U.S. Drug Enforcement Administration. (n.d.). Drug scheduling. Retrieved March 20, 2026, from https://www.dea.gov/drug-information/drug-scheduling
U.S. Food and Drug Administration. (n.d.). Opioid patient prescriber agreement (PPA). Retrieved March 20, 2026, from https://www.fda.gov/files/drugs/published/Opioid-Patient-Prescriber-Agreement-(PPA).pdf
U.S. Food and Drug Administration. (2020). Nonsteroidal anti-inflammatory drugs (NSAIDs): Drug safety communication—Avoid use of NSAIDs in pregnancy at 20 weeks or later. https://www.fda.gov/safety/medical-product-safety-information/nonsteroidal-anti-inflammatory-drugs-nsaids-drug-safety-communication-avoid-use-nsaids-pregnancy-20
U.S. Food and Drug Administration. (2024). FDA innovation challenge: Devices to prevent and treat opioid use disorder. https://www.fda.gov/about-fda/cdrh-innovation/fda-innovation-challenge-devices-prevent-and-treat-opioid-use-disorder
U.S. Food and Drug Administration. (2025). Pregnancy and lactation labeling resources. https://www.fda.gov/drugs/labeling-information-drug-products/pregnancy-and-lactation-labeling-drugs-final-rule
U.S. Preventive Services Task Force. (2022). Aspirin use to prevent cardiovascular disease: US Preventive Services Task Force Recommendation Statement. JAMA, 327(16), 1577–1584. https://doi.org/10.1001/jama.2022.4983
Wager, T. D. (2022). Managing pain. Cerebrum, 2022, cer-03-22. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9224345
Wald, A., & Johnston, C. (2024). Treatment and prevention of herpes simplex virus type 1 in immunocompetent adolescents and adults. UpToDate. Retrieved March 20, 2026, from https://www.uptodate.com/contents/treatment-and-prevention-of-herpes-simplex-virus-type-1-in-immunocompetent-adolescents-and-adults
Wheeler, S. G., Jarvik, J. G., & Chou, R. (2026). Evaluation of low back pain in adults. UpToDate. Retrieved March 20, 2026, from https://www.uptodate.com/contents/evaluation-of-low-back-pain-in-adults
Yu, H. H. M., & Hoffe, S. E. (2025). Overview of therapeutic approaches for adult patients with bone metastasis from solid tumors. UpToDate. Retrieved March 19, 2026, from https://www.uptodate.com/contents/overview-of-therapeutic-approaches-for-adult-patients-with-bone-metastasis-from-solid-tumors
Powered by Froala Editor