This learning activity aims to ensure that nurses working in various settings understand standard and transmission-based precautions and the proper use of personal protective equipment according to the Centers for Disease Control and Prevention guidelines to disrupt the chain of infection, including the different types of personal protective equipment and how to don and doff personal protective equipment properly.
Course preview
Personal Protective Equipment
Disclosure Statement
This learning activity aims to ensure that nurses working in various settings understand standard and transmission-based precautions and the proper use of personal protective equipment according to the Centers for Disease Control and Prevention guidelines to disrupt the chain of infection, including the different types of personal protective equipment and how to don and doff personal protective equipment properly.
Upon completion of this activity, learners should be able to:
- discuss the elements of the chain of infection, and identify the modes and mechanisms of pathogen transmission in the health care environment
- explain how to minimize a healthcare professional’s risk of acquiring an infectious disease
- identify and define standard and transmission-based precautions and associated HCP and patient implications
- consider the latest Centers for Disease Control and Prevention health care professionals’ guidelines for protection from infectious disease
- identify the proper selection and use of personal protective equipment and barriers to prevent patient and healthcare professional contact with potentially infectious material
Healthcare professionals (HCPs) risk contracting infectious diseases each time they enter their workplace. Proper infection control practices within the health care setting are a primary responsibility for all HCPs. In nursing, this responsibility affects all interactions with patients, coworkers, equipment, and the health care environment (Potter et al., 2023). It encompasses adherence to the following essential infection control practices:
- scientifically accepted standards for handwashing
- aseptic technique, including the use of gloves and other barriers for preventing bidirectional contact with blood and body fluids
- thorough cleaning followed by sterilization or disinfection of medical devices
- disposal of non-reusable materials and equipment
- cleaning of objects between patients that are visibly contaminated or subject to touch contamination with blood or body fluids
- injury prevention techniques or engineering controls to reduce the opportunity for patient and employee exposures (Potter et al., 2023)
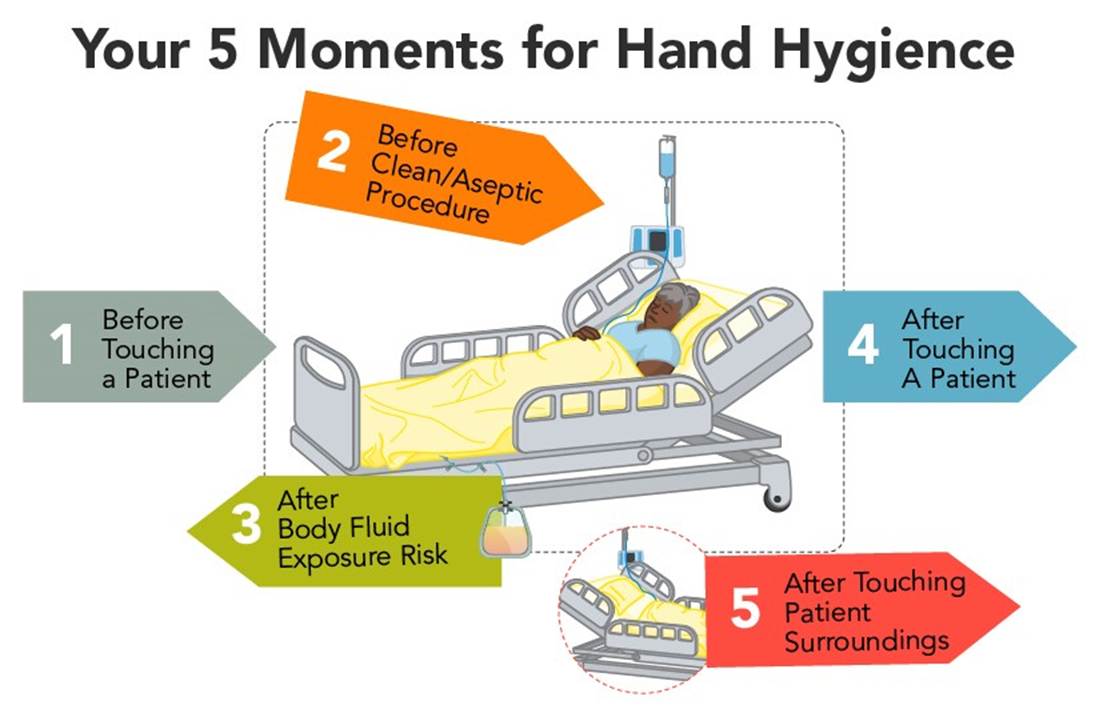
Adherence can be increased with frequent and high-quality training to understand how infection control strategies are effective and why they are necessary, such as the multimodal clean hands campaign developed by the World Health Organization’s (WHO) five Moments for Hand Hygiene (refer to Figure 1). Consequences of nonadherence include increased health risks for HCPs, patients, and the public, such as increased infection rates and antimicrobial resistance, as well as increased health care costs. Hand hygiene is a requirement, not a luxury, and saves millions of lives per year (WHO, 2009, 2023).
Figure 1
Five Moments for Hand Hygiene
Minimizing Risk for Exposure
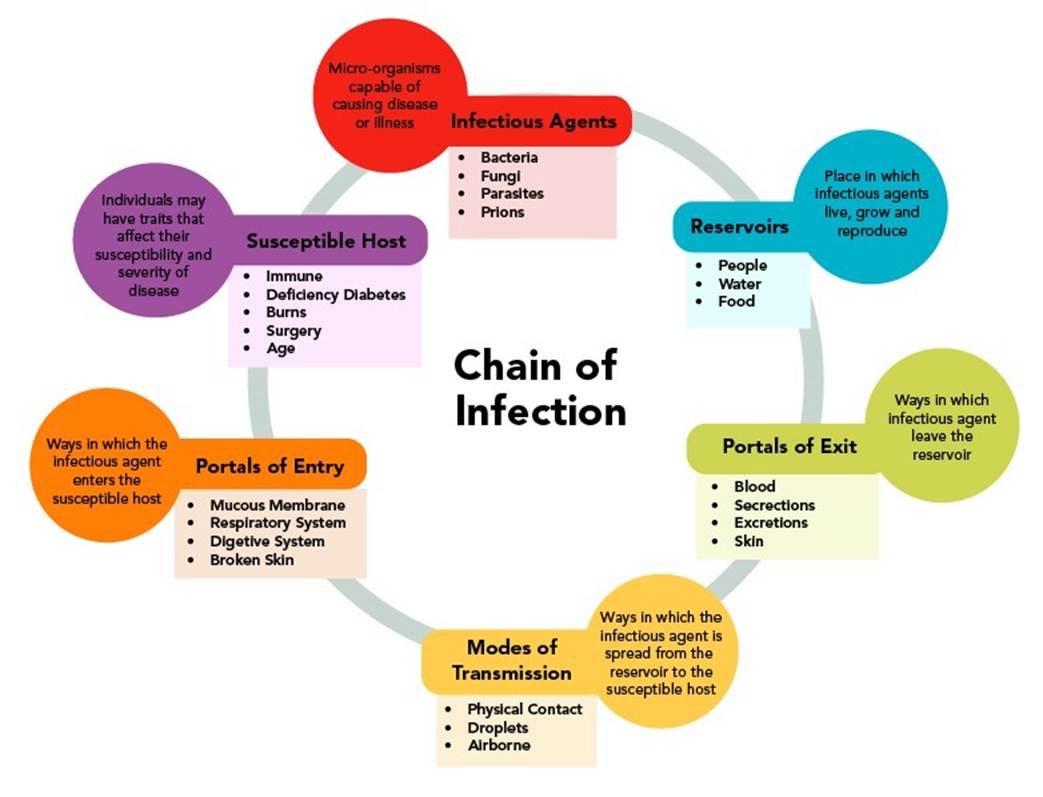
Handwashing is the most effective way to decrease disease transmission. HCPs have a higher risk of exposure to disease than through the hands alone; therefore, hand hygiene alone is insufficient protection. HCPs are exposed through direct contacts, such as touching; indirect contacts, such as equipment, eating utensils, or other vectors or vehicles of transmission; droplet transmission, such as coughing, sneezing, or spitting from the source to the eyes, nose, or mouth of others; or airborne transmission with the spread of microorganisms by dust particles or tiny droplets. Microorganisms enter the host through a portal of entry (usually the respiratory system). Portals of entry include skin, blood, and the respiratory, gastrointestinal, reproductive, and genital tracts. Frequently, microorganisms enter the host’s body by the same route they exited the source. HCPs use personal protective equipment (PPE) to decrease the risk of exposure by limiting the ability of microorganisms to enter their bodies. PPE includes gloves, respirators, facemasks, eyewear, and gowns to prevent the transmission of infectious materials found in blood, body fluids, secretions, and excretions (Centers for Disease Control and Prevention [CDC], 2025; Rogers & Brashers, 2023, pp. 281-283; WHO, 2009). Refer to Figure 2 for the chain of infection.
Figure 2
Chain of Infection
Standard and Transmission-Based Precautions
The CDC organizes precautions to prevent the transmission of infectious agents into two primary tiers: standard precautions and transmission-based precautions. Standard precautions are the basis of infection control practices and are of utmost importance to prevent the transmission of infectious agents and communicable diseases in health care settings. Standard precautions are applied to all patients in health care settings (regardless of the suspected or confirmed presence of an infectious agent). They are the first line of defense to break the chain of infection and protect HCPs and patients. Standard precautions are based on the concept that every patient’s blood or body fluids are potentially contaminated with infectious agents. Standard precautions are used when contact with blood, blood products, body fluids, secretions, excretions (except sweat), non-intact skin, or mucous membranes is...
...purchase below to continue the course
kely. Providing care using standard precautions includes hand hygiene; applying gloves, gown, facemask, or face shield; respiratory hygiene/cough etiquette; and safe injection practices. The selection of PPE depends upon anticipated blood, body fluid, or splash exposure (CDC, 2024c; Siegel et al., 2024, pp. 68–72).
In 2013, the CDC recommended incorporating respiratory hygiene/cough etiquette into infection control as a component of standard precautions. These should be instituted in the health care setting at the first point of contact with a potentially infected person to prevent the transmission of all respiratory infections. The recommended practices have a strong evidence base. Respiratory hygiene/cough etiquette applies to anyone entering a health care setting (patients, visitors, staff) with signs or symptoms of illness (cough, congestion, rhinorrhea, or increased production of respiratory secretions). The components of respiratory hygiene/cough etiquette include the following:
- covering the mouth and nose during coughing and sneezing
- using disposable facial tissues to contain respiratory secretions, with prompt disposal into a hands-free receptacle
- wearing a surgical mask when coughing to minimize contamination of the surrounding environment
- turning the head when coughing and staying at least 3 feet away from others, especially in common waiting areas
- washing hands with soap and water or alcohol-based hand rub after contact with respiratory secretions (CDC, 2024c; Siegel et al., 2024, pp. 68–72)
Transmission-based precautions are the second tier of infection control and are intended for use alongside the standard precautions described above. Transmission-based precautions are reserved for patients suspected of being infected or colonized with specific infectious agents that require additional precautions to prevent transmission. Also referred to as isolation precautions, transmission-based precautions are based on the infectious organism’s mode of transmission. Corresponding to the primary modes of transmission discussed earlier, the major categories of transmission-based protection include contact, droplet, and airborne precautions. These are used for patients with highly transmissible pathogens when the route of transmission is not entirely interrupted by standard precautions. Regardless of the specific type of transmission-based precautions required, the following principles should be routinely adhered to:
- thoroughly perform hand hygiene before entering and leaving the room of a patient in isolation
- properly dispose of contaminated supplies and equipment according to agency policy
- apply knowledge of the mode of infection transmission when using PPE
- protect all persons from exposure during the transport of an infected patient outside of the isolation room
- single private rooms are preferred when available, but cohorting may be implemented during outbreaks of infections (i.e., the placement of patients infected with the same organism in the same room based on organizational needs; CDC, 2024d; Siegel et al., 2024, pp. 72-76)
Contact precautions are used when a disease is transmitted via direct contact, contaminated body fluids, or indirectly through contaminated instruments, equipment, or the hands of HCPs. This precaution requires wearing gloves and a gown for all interactions involving contact with the patient or potentially contaminated areas in the patient’s environment. These patients should also be in a private room with a private bathroom to prevent cross-contamination. Examples of infections in which contact precautions are instituted include vancomycin-resistant Enterococcus (VRE), methicillin-resistant Staphylococcus aureus (MRSA), Clostridioides difficile (C. diff), respiratory syncytial virus (RSV), norovirus, and rotavirus. Contact precautions may also apply in situations where there is severe wound infection/drainage, fecal incontinence, or other discharges from the body that may increase the risk of contamination of the environment and overall risk of transmission of the infectious agent (CDC, 2024d; Siegel et al., 2024, pp. 17-18, 73).
Droplet precautions are used when a disease is transmitted by large droplets expelled into the air. They are typically larger than 5 µm and can travel an estimated 3–6 feet from the patient. This precaution requires the HCP to apply a surgical mask when within close proximity of the patient (or before entering the patient’s room) and use dedicated care equipment. Patients requiring droplet precautions include those with suspected or confirmed influenza, pertussis, meningococcal disease, adenovirus, group A streptococcus, or rhinovirus (CDC, 2024d; Siegel et al., 2024, pp. 19, 73–74).
Airborne precautions are used when a disease is transmitted by smaller droplets (typically less than 5 µm). These droplets can remain airborne for extended periods. If possible, the patient should be placed in a private room with negative pressure airflow. This airflow filters air through a high-efficiency particulate air (HEPA) filter and then directs the air to the outside of the facility. This form of isolation requires a respirator, gown, and gloves to be applied before entering the patient’s room. Respirators must be appropriately fitted before use. Examples of diagnoses requiring airborne precautions are Mycobacterium tuberculosis, rubeola (measles), varicella-zoster (chickenpox), and severe acute respiratory syndrome (SARS; CDC, 2024d; Siegel et al., 2024, pp. 20, 29, 74–75). With all types of transmission-based precautions, certain basic principles should be followed:
- thoroughly perform hand hygiene before entering and leaving the room of a patient in isolation
- properly dispose of contaminated supplies and equipment according to agency policy
- apply knowledge of the mode of infection transmission when using PPE
- protect all persons from exposure during the transport of an infected patient outside of the isolation room (CDC, 2024c, 2024d)
Types of Personal Protective Equipment
Gloves
Gloves should be worn when there is the potential for contact with patients who have infectious agents transmitted by contact, in anticipation of contact with any infectious material, and when touching possibly contaminated equipment or surfaces. Disposable gloves are made from various polymers such as latex, nitrile, and vinyl. Both nonsterile and sterile gloves are used by HCPs when delivering care to patients. Gloves should be selected based on the task, anticipated contact with certain agents, size, latex sensitivities, and facility policy. Latex and nitrile gloves have been shown to offer superior protection against pathogens, compared to vinyl gloves, making them the preferred choice when extended patient contact is anticipated (Siegel et al., 2024, pp. 52-53).
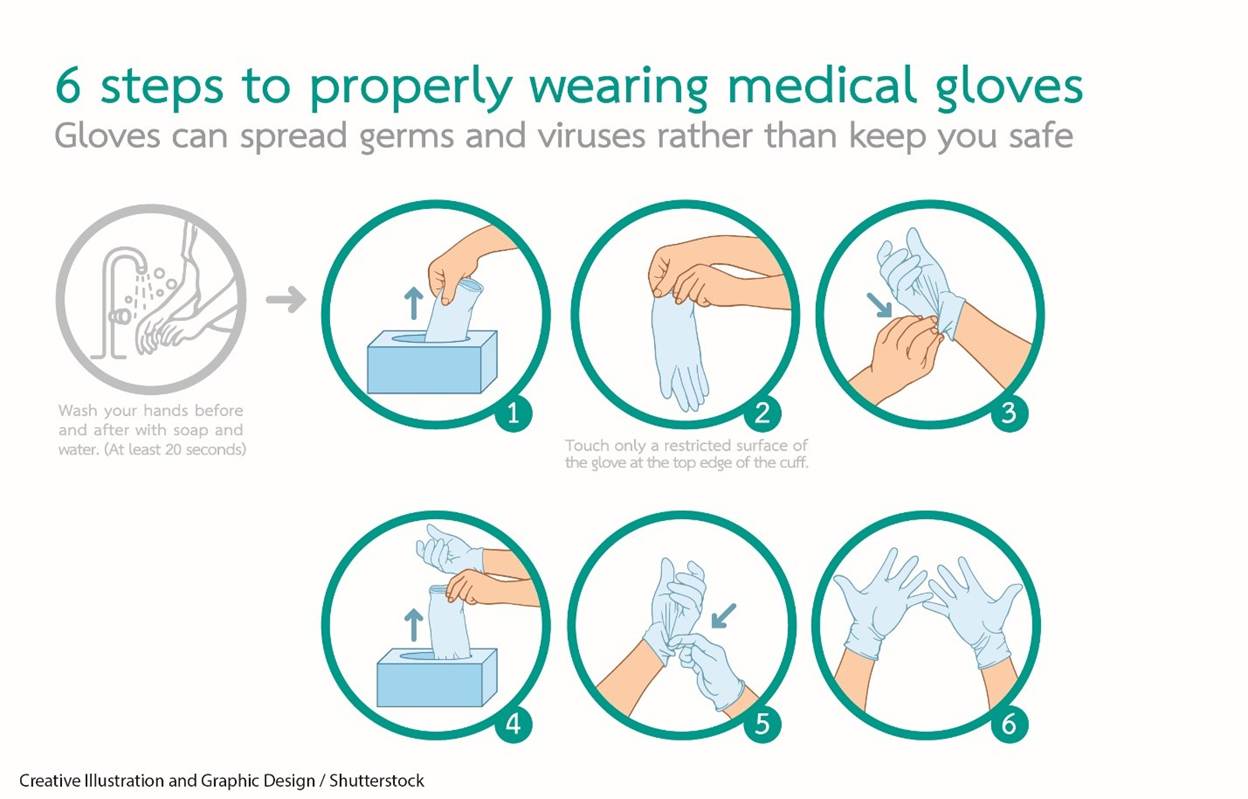
The following are essential points to consider when using gloves. Wear clean gloves when touching blood, body fluids, secretions, excretions, and contaminated items. Apply gloves before touching mucous membranes and non-intact skin. Gloves should fit comfortably and never be reused. The use of gloves does not eliminate the need for hand hygiene. Likewise, completing hand hygiene does not eliminate the need for gloves. Change gloves between tasks and procedures on the same patient after contact with a material that may contain a high concentration of microorganisms. Remove gloves promptly after use, before touching non-contaminated items and environmental surfaces, and before going to another patient or leaving the room. Wash hands immediately to avoid transferring microorganisms to other patients or environments (CDC, 2024a; Potter et al., 2023). The procedure for the proper application of nonsterile gloves is as follows (refer to Figure 3):
- perform hand hygiene until the product disappears and the hands are dry
- select the appropriate size glove
- holding the glove at the opening, slip the fingers into the glove and pull tight
- with the gloved hand, hold the second glove at the opening and slip the ungloved fingers into the glove and pull tight
- pull gloves to the wrists of both hands (Potter et al., 2023; Siegel et al., 2024, p. 132)
Figure 3
Proper Application of Nonsterile Gloves
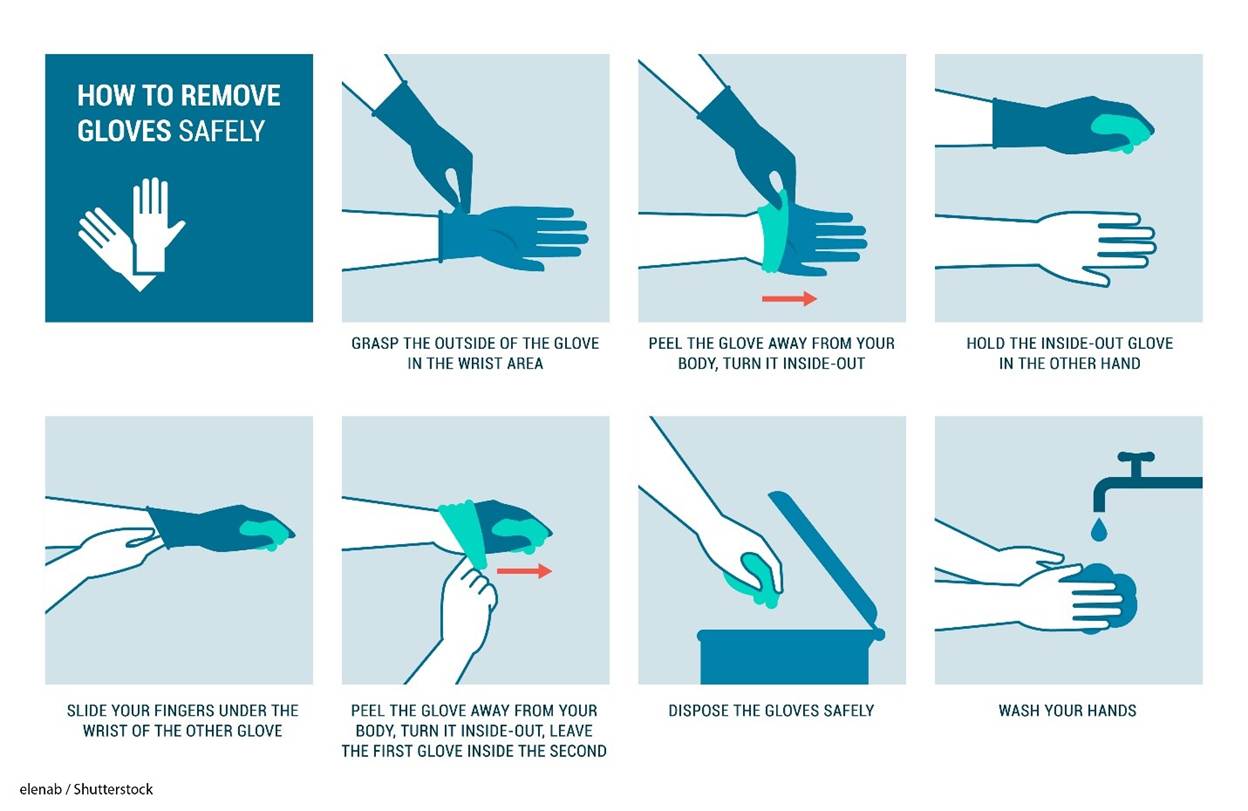
The procedure for the proper removal of nonsterile gloves is as follows (refer to Figure 4):
- remove the gloves by grasping the outside surface of the cuff of one hand using the other gloved hand
- avoiding skin contact, roll the first glove inside out and place it in the palm of the gloved hand
- grasp the second glove on the inside of the cuff and pull it inside out
- dispose of both gloves
- perform hand hygiene (CDC, 2024b; Potter et al., 2023; Siegel et al., 2024, p. 133)
Figure 4
Proper Removal of Nonsterile Gloves
Latex and Latex-Free Equipment
The use of latex gloves by HCPs increased in the late 1990s due to new standards released by the U.S. Occupational Safety and Health Administration (OSHA), which required protective glove use. This led to a shortage of latex and the need to tap younger trees to acquire latex, and the use of stimulants. The combination of this with increased overall glove usage resulted in a significant increase in the rate of latex sensitivity/allergies. After this occurred, the avoidance of latex gloves in many hospital systems resulted in fewer incidences of latex allergies. Despite a lower prevalence of latex allergies, HCPs and patients who have received multiple surgeries remain high-risk groups. Exposure to latex can lead to the development of contact dermatitis, urticaria, rhinoconjunctivitis, asthma exacerbation, and anaphylaxis. Powdered latex gloves create an additional risk because the latex allergen adheres to the powder and can become airborne and inhaled into the lungs as the latex glove is used (Hamilton, 2025; Potter et al., 2023).
The primary treatment for latex allergies is avoidance. HCPs and patients should refrain from contact with latex-containing products, even if treatments such as immunotherapy and anti-immunoglobulin E are trialed. HCPs with latex allergies are protected under the Americans with Disabilities Act. Individuals with a sensitivity or allergy to kiwifruit, papaya, avocado, banana, potato, chestnut, or tomato should be carefully screened, as they are at a higher risk of developing a sensitivity or allergy to latex (Hamilton, 2025; Potter et al., 2023).
Facemasks
Facemasks provide barriers to infectious materials and are often used with other PPE, such as gowns and gloves. Masks should be worn to protect the HCP from infectious material from the patient, when sterile technique is required to protect the patient, and as part of cough etiquette/respiratory hygiene among coughing patients. When worn correctly, facemasks and eye protection protect the mouth, nose, and eyes during procedures where there is a potential for blood or body fluids to splash or spray. The mucous membranes of these areas are susceptible to infectious agents. The use of facemasks during certain procedures falls under the definition of standard precautions. Examples of such procedures include suctioning, bronchoscopy, lumbar punctures, insertion of catheters, and invasive vascular procedures. In addition to these standard precautions, a mask should be worn by HCPs when caring for patients who require droplet precautions. A surgical or procedure mask should not be confused with a respirator, which will be reviewed in more detail (Potter et al., 2023; Siegel et al., 2024, pp. 54–55, 70, 74).
Procedure (i.e., surgical) facemasks are flat, pleated, and affixed to the head with ear loops. They are used for any nonsterile procedure. These masks come in two basic types: one that is affixed to the head with two ties and may be flat/pleated or duck-billed in shape; the other type has an elastic loop for each ear. Both conform to the face with a flexible strip for the bridge of the nose that can be manually adjusted by pinching. All facemasks have some degree of fluid resistance. However, those approved as surgical masks must meet specific standards by the U.S. Food and Drug Administration (FDA) to protect against blood and body fluid penetration. Surgical masks protect the HCP from sprays or splashes and prevent pathogens within the wearer’s nose or mouth from potentially spreading to and infecting the patient (CDC, 2022; Potter et al., 2023; Siegel et al., 2024, p. 55). The steps for properly applying a surgical mask are as follows (refer to Figure 5):
- place and hold the surgical mask over the nose, mouth, and chin while stretching the band over the ears or tying the ties behind the head and at the base of the neck
- adjust the surgical mask so it is snug with no gaps; the surgical mask should not be touched or readjusted during use (Potter et al., 2023)
Figure 5
Applying a Surgical Mask

(Lara / Shutterstock)
The steps for properly removing a surgical mask are as follows (refer to Figure 6):
- after properly removing and disposing of gloves, carefully remove the elastic from the ears or untie the surgical mask from the back of the head, bottom tie first, being sure to avoid touching the front of the facemask with your bare hands
- dispose of the surgical mask
- finally, perform hand hygiene (Potter et al., 2023; Siegel et al., 2024, pp. 132–133)
Figure 6
Removing a Surgical Mask

Respirators
Respirators cover the nose and mouth with N95 protection or higher to prevent airborne transmission of infectious agents. These reduce the HCP’s risk of inhaling hazardous airborne particles, gases, or vapors. Respirators are reserved for case-specific aerosolizing procedures where airborne particulates create a high risk of infection for the HCP. OSHA standards require that National Institute for Occupational Safety and Health (NIOSH)-approved N95 filtering facepiece respirators or higher be used when in contact with patients with certain suspected or confirmed airborne-transmitted diseases, such as tuberculosis or measles. In addition, these masks must meet requirements to filter a minimum of 95% of 0.3 µm-size particles and require fit testing. Most N95 respirators are single-use and disposable (refer to Figure 7), which tend to be lighter and less cumbersome for the wearer. Reusable options include elastomeric and powered air-purifying respirators (PAPR; refer to Figure 8). Some of these options have the advantage of also providing face and eye protection in one unit, as well as reducing the risk of self-contamination. Respirators are intended for protection against solids; they are highly durable devices and have a soft and comfortable inner surface, adjustable nosepiece, and secure head straps to provide a proper fit (CDC, 2022; Potter et al., 2023; Siegel et al., 2024, pp. 56–57).
Figure 7
N95 Mask

Figure 8
Powered Air-Purifying Respirator (PAPR)

There are fundamental differences between the major forms of respiratory protection used in health care settings: a surgical mask, a filtering facepiece respirator, and a PAPR. While surgical masks are cleared by the FDA, both respirators are evaluated, tested, and approved in the United States by the NIOSH based on specific federal requirements. A surgical mask is disposable and loose-fitting, but it protects HCPs from splashes, sprays, and droplets because it is fluid-resistant. It also protects the public (i.e., patients) from the HCP’s respiratory emissions. They do not require a fit test and do not provide reliable respiratory protection for the HCP from smaller airborne particles due to leakage around the edge of the mask when the HCP inhales. A filtering facepiece respirator, such as an N95 mask, is tight-fitting and protects the HCP from exposure to large droplets and small particle non-oil aerosols (at least 95% of airborne particles of 0.3 µm and larger). N95s were intended to be discarded after each patient encounter, after aerosol-generating procedures, when damaged/deformed, wet, visibly soiled, or contaminated with bodily fluids. A half-facepiece respirator is constructed of rubber or synthetic materials, making it reusable and tight-fitting. They should be cleaned and disinfected between each patient encounter. The associated filter blocks 95%, 99%, or 99.97% of small particles, vapors, or gases. Both types of respirators require fit testing to ensure a proper seal for the HCP and consequent respiratory protection (CDC, 2022; Siegel et al., 2024, pp. 20, 56–57).
Face and Eye Protection
Protective goggles, face shields, and safety glasses provide a barrier to infectious substances. They are typically used with other PPE, such as gloves, gowns, respirators, and facemasks. The type of face and eye protection chosen depends on the specific work conditions and potential for exposure. Personal knowledge of potential exposure is essential for making an informed decision about the best face and eye protection. Eyeglasses prescribed for vision correction and contact lenses are not considered eye protection. Evaluating the combination of PPE recommended for the specific work situation is essential for complete and proper protection. For example, some facemasks may not work with specific goggles or shields. Likewise, a full-face respirator may provide adequate protection without additional components of PPE (Potter et al., 2023; Siegel et al., 2024, pp. 54–56).
Safety glasses are excellent for providing impact protection. However, they do not protect adequately from splashes, sprays, and respiratory droplets. Thus, they are not typically used for infection control. Goggles are available with direct or indirect venting. Direct-vented goggles have the potential to allow the penetration of splashes and are not as reliable as indirect-vented goggles. Goggles must fit snugly to provide adequate protection from splashes, sprays, and respiratory droplets. Newer goggles even have properties to reduce fogging (Potter et al., 2023; Siegel et al., 2024, pp. 55–56). The proper steps for applying safety goggles are as follows (refer to Figure 9):
- grasp the temples (long arms) of the goggles, spread the temples open, and slowly place them over the ears
- if needed, adjust the goggles for comfort (Potter et al., 2023)
Figure 9
Applying and Adjusting Goggles

The proper steps for removing and disposing of goggles are as follows:
- after removing and discarding gloves, grasp the earpieces and lift them away from the face, being sure to avoid touching the front of the goggles with bare hands
- discard disposable goggles in the appropriate receptacle; if the goggles are designed to be reused, clean and store them according to agency protocol (Potter et al., 2023; Siegel et al., 2024, p. 133)
Face shields are sometimes used as an alternative to goggles or safety glasses. Since the face shield has a larger surface area, it protects other facial areas in addition to the eyes. Face shields do not fit snugly against the face, making them vulnerable to splash and spray particles that can easily penetrate beneath the shield. Therefore, face shields are typically used with other forms of protection and should not be considered the best protection when used alone (Potter et al., 2023; Siegel et al., 2024, p. 56).
Gowns
A clean, nonsterile gown protects skin and prevents the soiling of clothing during procedures and patient-care activities that are likely to generate splashes or sprays of blood, body fluids, secretions, or excretions. Most patient interactions do not require a gown, but they are always needed when caring for patients on contact isolation precautions and should always be worn in combination with gloves. Select a gown appropriate for the activity and the amount of fluid likely to be encountered; gowns are tested and determined to be either fluid-resistant or impervious. Remove a soiled gown as soon as possible and complete hand hygiene to avoid transferring microorganisms to other patients or equipment (Potter et al., 2023; Seigel, 2024, pp. 53–54). The steps for donning a gown are as follows (refer to Figure 10):
- select the appropriate type and size of gown
- with the gown opening toward the back, put arms through the sleeves one at a time and pull the gown over the shoulders; secure the gown at the neck and waist using the provided closure mechanism (Potter et al., 2023)
Figure 10
Donning a Gown

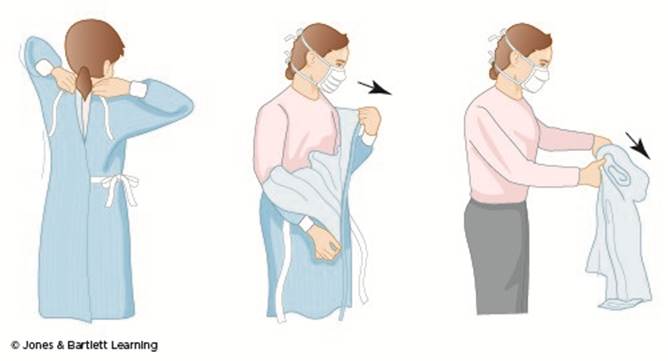
To prevent clothing and equipment contamination, the gown must be properly removed. The steps for doffing a gown are as follows (refer to Figure 11):
- if the gown is disposable, gloves may be rolled into the gown during the removal of the sleeves to prevent contamination; if using a washable gown, remove gloves first (following the removal steps in Figure 4)
- untie the gown at the neck, then waist, and pull it away from the shoulders; roll it into a bundle while avoiding contact with the outside of the gown
- if the gown is disposable, place it in the appropriate waste container after removal; if the gown is reusable, place it in the proper soiled laundry container after removal
- regardless of the type of gown used, perform hand hygiene following removal (Potter et al., 2023; Seigel, 2024; pp. 54, 133)
Figure 11
Doffing a Gown
Proper Donning and Doffing of Personal Protective Equipment
Adhering to the proper sequence of donning and doffing PPE is vital to reducing the spread of microorganisms. The graphic examples shown in Figures 12 and 13 demonstrate the CDC’s recommendations for both tasks. Proper doffing of PPE is essential to prevent self-contamination during removal. Since more than one method may be acceptable, HCPs must consult the training and practices outlined by their institution’s policies and procedures (CDC, 2023; Siegel et al., 2024, pp. 132–133).
Figure 12
Applying Personal Protective Equipment
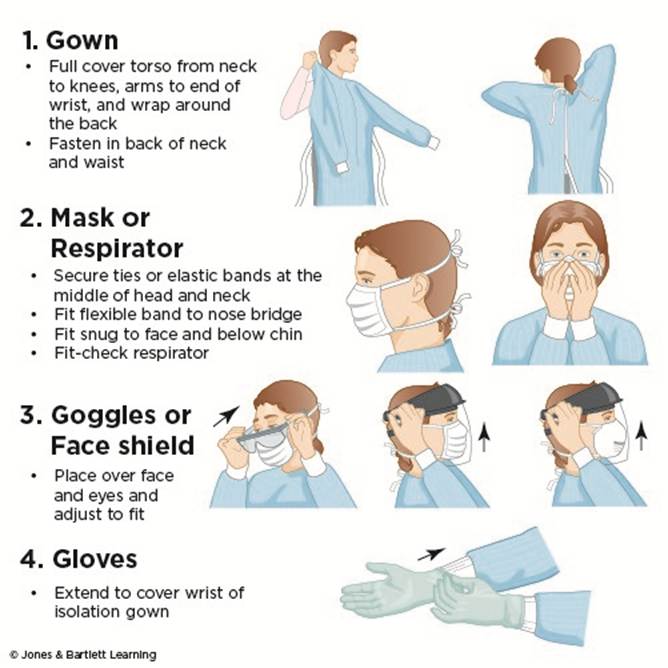
Figure 13
Removing Personal Protective Equipment
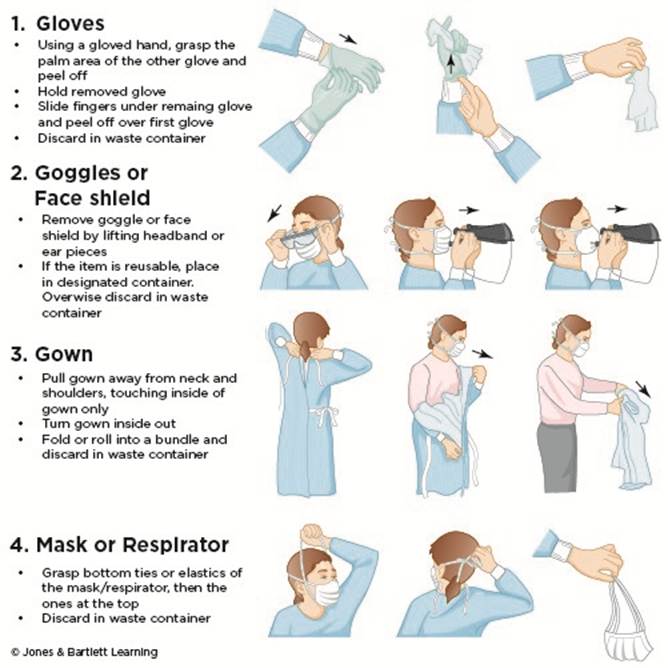
Alternatively, if the HCP is wearing disposable gloves that extend on top of the cuff of the disposable gown, the HCP can pull forward on the front of the gown, causing the ties in the back to break. The HCP should ensure that they touch only the outside of the gown using their gloved hands during this maneuver. The HCP should then remove the gown, folding or rolling it inside out or into a bundle. When removing the gown from the wrist, the HCP should peel off the gloves from the hands at the same time, touching only the inside of the gown/gloves with their bare hands. After leaving the patient’s room, the mask or respirator can then be removed. Remember that the front and sleeves of the gown, the outside of the gloves, the outside/front of the goggles or face shield, and the front of the mask/respirator are expected to be contaminated. If the HCP contaminates their bare hands during PPE removal at any point, they should stop and wash their hands or use an alcohol hand sanitizer before proceeding. Following any PPE removal, hand hygiene should be performed as described previously (CDC, 2023; Siegel et al., 2024, pp. 52-57).
***For further information on infection control outside the use of PPE, please refer to NursingCE’s module on Infection Control.
References
Centers for Disease Control and Prevention. (2022). Hospital respiratory protection program toolkit: Resources for respiratory program administrators. https://www.cdc.gov/niosh/docs/2015-117/pdfs/2015-117revised042022.pdf?id=10.26616/NIOSHPUB2015117
Centers for Disease Control and Prevention. (2023). Appendix A: Figure. Example of safe donning and removal of personal protective equipment (PPE). Retrieved February 12, 2026, from https://www.cdc.gov/infection-control/hcp/isolation-precautions/appendix-a-figure.html
Centers for Disease Control and Prevention. (2024a). Clinical safety: Hand hygiene for healthcare workers. Retrieved February 11, 2026, from https://www.cdc.gov/clean-hands/hcp/clinical-safety/index.html
Centers for Disease Control and Prevention. (2024b). How to remove gloves safely. Retrieved February 11, 2026, from https://www.cdc.gov/ebola/hcp/communication-resources/how-to-remove-gloves-safely.html
Centers for Disease Control and Prevention. (2024c). Standard precautions for all patient care. Retrieved February 11, 2026, from https://www.cdc.gov/infection-control/hcp/basics/standard-precautions.html
Centers for Disease Control and Prevention. (2024d). Transmission-based precautions. Retrieved February 11, 2026, from https://www.cdc.gov/infection-control/hcp/basics/transmission-based-precautions.html
Centers for Disease Control and Prevention. (2025). Infection control basics. Retrieved February 12, 2026, from https://www.cdc.gov/infection-control/about/index.html
Hamilton, R. G. (2025). Latex allergy: Epidemiology, clinical manifestations, and diagnosis. UpToDate. Retrieved February 11, 2026, from https://www.uptodate.com/contents/latex-allergy-epidemiology-clinical-manifestations-and-diagnosis
Potter, P. A., Perry, A. G., Stockert, P. A., & Hall, A. M. (2023). Fundamentals of nursing (11th ed.). Elsevier.
Rogers, J. L. and Brashers, V. L. (Eds.). (2023). McCance and Huether's pathophysiology: The biologic basis for disease in adults and children (9th ed.). Elsevier.
Siegel, J. D., Rhinehart, E., Jackson, M., Chiarello, L., & The Healthcare Infection Control Practices Advisory Committee. (2024). 2007 guideline for isolation precautions: Preventing transmission of infectious agents in healthcare settings. https://www.cdc.gov/infection-control/media/pdfs/guideline-isolation-h.pdf
World Health Organization. (2009). Hand hygiene technical reference manual: To be used by health-care workers, trainers and observers of hand hygiene practices. https://www.who.int/publications/i/item/9789241598606
World Health Organization. (2023). Key facts and figures: World hand hygiene day 2023. https://www.who.int/campaigns/world-hand-hygiene-day/2021/key-facts-and-figures
Powered by Froala Editor