About this course:
This course provides an overview of the types, causes, and risks of medical errors and their impact on patient outcomes. In addition, this course explores the nurse’s role and responsibilities in preventing errors and describes the key aspects of a culture of safety.
Course preview
Prevention of Medical Errors
This course provides an overview of the types, causes, and risks of medical errors and their impact on patient outcomes. In addition, this course explores the nurse’s role and responsibilities in preventing errors and describes the key aspects of a culture of safety.
Upon completion of this module, learners should be able to:
- define important terminology related to medical errors
- discuss the incidence of medical errors
- identify common types of medical errors
- understand the nurse’s role and responsibilities in preventing medical errors
- review the root cause analysis (RCA) in the identification of medical errors
- summarize The Joint Commission’s (TJC) national performance goals (NPGs) related to medical errors
- describe the key aspects of a culture of safety
Medical errors include events caused by omission or commission and occur during the planning or execution of medical services. Medical errors are recognized as a serious public health concern for both patients and health care organizations, as they lead to poor patient outcomes and increase the cost of health care delivery. Since the landmark publication To Err Is Human: Building a Safer Healthcare System was introduced in 2000 by the National Academies Press, formerly known as the Institute of Medicine (IOM), health care organizations have taken a deeper look at the number of medical errors occurring annually and the need to improve the quality and safe delivery of patient care (IOM, 2000).
It has been reported that medical errors are often unrecognized, even though reported medical errors lead to more than 200,000 deaths annually in the United States. This number exceeds the number of deaths caused by stroke, chronic lower respiratory disease, Alzheimer’s disease, and diabetes mellitus (DM), according to the National Center for Health Statistics (NCHS). Medical errors are the fourth leading cause of death in the United States, behind heart disease, cancer, and unintentional injuries. The number of deaths due to medical errors is likely higher, being underrecognized due to a lack of identification and reporting. There is no ICD-10 code for medical errors; therefore, a medical error cannot be selected as a potential cause of death on death certificates. Since the Centers for Disease Control and Prevention’s (CDC) collection of national health statistics is based on the listed cause of death on death certificates, available data do not adequately capture the significance of the problem (Murphy et al., 2024; Rodziewicz et al., 2024).
An estimated 400,000 hospitalized patients are victims of some preventable harm or death each year. Beyond the emotional and physical tolls of medical errors, the monetary cost is estimated to be between $20 billion and $45 billion annually. Expenses related to medical errors include increased length of hospital stay, prescription drug costs, outpatient care, lost work, and lost productivity. Patient safety can be improved by identifying the factors that contribute to medical errors and using this data to develop multifaceted prevention protocols across various health care organizations. With the implementation of various medical error prevention protocols, the Agency for Healthcare Research and Quality (AHRQ) National Scorecard has reported a downward trend in hospital-associated conditions (HAC), including hospital-associated infections (HAIs), falls, and pressure injuries. These protocols, including focused patient safety interventions, have saved up to $7.7 billion in health care costs and prevented more than 20,000 hospital deaths (AHRQ, 2019; Lodato et al., 2025; Rodziewicz et al., 2024).
Most health care providers (HCPs) recognize the significance of medical errors and their threat to patient safety and outcomes. Nurses must recognize their role in preventing medical errors and be accountable for their actions. Nurses are crucial in maintaining a culture that fosters patient safety and are responsible for recognizing potential opportunities to promote positive change that safeguards care. Also, nurses are well positioned to educate the entire health care team and the public on identifying risks, preventing medical errors, and properly reporting and reconciling medical errors or near misses. Nurses must recognize and report any medical errors or adverse events to remain accountable. This may be difficult due to the psychological effects of causing a medical error. Responsible individuals can feel inadequate, depressed, angry, and even suicidal depending on the extent and patient outcome resulting from the medical error. Since most HCPs went into the profession to help patients, individuals can feel like they failed their patients when poor outcomes occur due to medical errors, in addition to the fear of legal repercussions (Lancaster et al., 2022; Rodziewicz et al., 2024; Yılmaz & Sönmez, 2024).
Common Medical Errors
Throughout the literature, various terms are associated with adverse health care events and medical errors. While the categories listed in Table 1 may overlap, they are the most commonly addressed medical errors across the health care continuum.
Table 1
Common Medical Errors
Medical Error | Explanation |
Active error | Occurs between an individual and an aspect of the larger health system; a frontline clinician makes these errors (e.g., administering the wrong drug) |
|
...purchase below to continue the course | A type of injury experienced by a patient; only preventable adverse events are considered a medical error |
Adverse drug event (ADE) | Occurs when a medication leads to patient harm; they are always unwanted and typically require intervention; they may be preventable or nonpreventable (often referred to as an adverse drug reaction [ADR] or side effect, which occur with normal use/dosing) |
Diagnostic error | Occurs when a diagnosis is missed, wrong, or delayed |
Falls | Occurs when an injury is sustained from an individual falling while health care personnel are present |
Iatrogenic infection | Includes any infection acquired during a health care contact or due to the care received during hospitalization |
Laboratory error | Consists of errors that lab personnel make during procedure performance, evaluation of data, reporting results of a test or procedure, or inaccurately recording the results of a test or procedure |
Latent error | A failure of organization or design, including systems, policies, procedures, or equipment; it often goes unnoticed without any detectable harm; when an active error occurs, it can uncover an unrecognized latent error (i.e., an accident waiting to happen) |
Medication error | A preventable event that can lead to the inappropriate use of medications or cause patient harm; it can occur when the medication is in the control of an HCP, patient, or consumer |
Medical misadventure | Includes ADRs (side effects), ADEs, and medication errors; it occurs through omission or commission of medication administration (explained further on) and is always undesirable |
Near miss (close call) | Any event that could have potentially led to an adverse event or patient harm but did not, either due to chance or some intervention; these situations provide opportunities for system and process improvements and should receive the same level of follow-up as an adverse event |
Negligence | Failure to meet or provide the expected standard of care |
Never event | An error that should never happen if standard practices are followed; there are 29 events in this group, including surgical events, product or device events, patient protection events, environmental events, radiologic events, and criminal events; these rare events are devastating to patients when they occur (e.g., a hospital may experience a wrong-site surgery every 5–10 years, but the event is overwhelming to the patient, staff, and organization) |
Pharmacy error | Can occur at multiple points, including the preparation or processing of a prescription or through patient education that may be inaccurate; this may include prescribing the wrong medication or at the wrong dosage, failing to recognize harmful interactions of medications, or marketing defective or unsafe medications; pharmacy errors are associated with workload, insufficient training, negligence in supervising pharmacy technicians, a poor work environment, and overreliance on automated systems for dispensing |
Surgical error | Encompass errors that should never occur, such as wrong-site, wrong-patient, or wrong-procedure errors (WSPEs), and identify a serious safety problem within a health care system or organization |
System or process error | Involves predictable human failings that are related to poorly designed systems |
Errors of omission | Errors of omission occur when an action is not taken, such as not administering medication when ordered or indicated based on a patient’s condition |
Errors of commission | Errors of commission occur when a drug is administered that is not ordered or is contraindicated for the patient |
(AHRQ, 2025; AHRQ Patient Safety Network [PSN], 2024c, 2024e, 2024g, 2024i; Boddy & Avery, 2023; Dawson, n.d.; National Coordinating Council for Medication Error Reporting and Prevention [NCCMERP], n.d.; Rodziewicz et al., 2024; Tariq et al., 2024; Zhu & Weingart, 2025)
Additional patient safety event terminology pertinent to this topic includes a no-harm event, in which there is no harm caused to the patient who encounters a patient safety event; a close call, which is a patient safety event that did not reach the patient; and a hazardous condition, which is a situation that increases the likelihood of an adverse event. These events are tracked and used as opportunities to identify problem areas within a system or process. Health care organizations use event reporting for no-harm, close-call, or hazardous conditions for comprehensive analysis, risk identification, and the development of a corrective action plan to avoid future occurrences (Griffin, 2023; The Joint Commission [TJC], n.d.-c).
Causative Factors
Medical errors are multifactorial, and multiple errors can occur within the same hospital stay. Despite the many influencing factors, according to the AHRQ, there are eight common root causes of medical errors (AHRQ, 2003). These are described in Table 2.
Table 2
Common Root Causes of Medical Errors
Root Cause | Example |
Communication problems | Verbal or written errors between the health care team, patient, or family |
Inadequate information flow | Necessary information does not follow the patient through the health care system; this may affect prescribing decisions, lack of communication about test results, or poor coordination of medication orders for transfer of care |
Human problems | Standards of care, policies, processes, or procedures are not followed correctly, such as poor documentation or labeling of specimens; individual health care workers may not have sufficient knowledge to deliver care |
Patient-related issues | This may include improper patient identification, inadequate patient assessment, failure to obtain consent, or insufficient patient education |
Organizational transfer of knowledge | Insufficient training or inadequate education for those delivering care to patients; new employees or temporary help need knowledge transfer to provide safe care |
Staffing patterns and workflow | Inadequate staffing puts health care workers in situations that could lead to mistakes, such as exhaustion, distraction, or time constraints |
Technical failures | Medical devices, grafts, implants, or equipment complications or failures |
Inadequate policies | Poor documentation, inadequate procedural directions, and nonexistent policies |
(AHRQ, 2003; Patel & Goldin, 2025; Rodziewicz et al., 2024)
While various sources outline the causes of medical errors, almost all rank communication as the top opportunity for upholding patient safety. From diagnosis to treatment, medication administration, following policies and procedures, or patient education, HCPs must effectively communicate with other health care team members, families, and patients. Communication may be written or verbal; errors can occur throughout information delivery by omission and commission. Any failure to communicate effectively leads to medical errors and may occur at the point of patient hand-off, in the delivery of care, or during discharge instructions. Patients or their families may be reluctant to verbalize when they need help understanding instructions or may not seek clarification. Furthermore, nurses may need more knowledge of a specific disease process or treatment to be more effective in delivering patient education. Interactions between providers that lead to the mishandling of critical patient information can also be a source of communication breakdown that results in patient errors or poor outcomes (Adler, 2026; AHRQ PSN, 2024d; Howick et al., 2024; Patel & Goldin, 2025; Rodziewicz et al., 2024).
The TJC has several focused solutions to improve patient hand-off and communication among HCPs and ultimately enhance processes and systems. Their Handoff Communications Targeted Solutions Tool® guides health care organizations through steps to:
- measure the organization’s current hand-off process
- identify barriers to success and provide a measurement system that creates data to support needed changes or system improvements
- guide the organization to effective solutions that will address their unique needs, along with customizable forms for data collection and guidelines for the optimum hand-off communication processes (TJC, n.d.-e; TJC Center for Transforming Healthcare, n.d.)
As previously noted, most medical errors are due to systemic or institutional failures, not individual negligence or incompetence. Systemic failures can involve inadequate policies and procedures, a failure to retain or train staff, a failure to adequately staff patient care units, a failure to obtain and maintain safe equipment or supplies for the delivery of care, or a failure to recognize and manage errors or the conditions that led to the errors. In today’s health care setting, a systems approach pioneered by British psychologist James Reason is most frequently used. His analysis of errors in industrial, aviation, and nuclear environments determined that catastrophic errors seldom occurred due to a single individual, but rather from serious underlying flaws of the overall system. His model, the Swiss Cheese Model, describes workplaces or systems with underlying flaws or “holes.” Errors made by individuals within the system can result in severe consequences due to these holes. Dr. Reason’s model explains how disasters can happen and result in a significant impact on the organization. He also describes how these holes can be identified and “shrunk” so they are not liabilities in the future. His work acknowledges that human error is inevitable, particularly in a fast-paced health care environment. A systems approach can allow for the recognition of errors before consequences develop. Dr. Reason defines the terms latent errors and active errors. An active error occurs at the point of contact between a human and some component of the larger system, such as a piece of equipment or a department. A latent error is an accident waiting to happen and is usually related to a design failure of an organization that leads to inevitable patient harm. Other terms related to systemic errors include sharp end and blunt end, which align with active and latent errors. Personnel at the sharp end are active in delivering the error, such as administering the wrong medication. The blunt end refers to the layers of the health care system that are behind the scenes and not in direct contact with patients but still influence the sharp end (AHRQ PSN, 2024g; Gregory & Kaprielian, n.d.; Wiegmann et al., 2022).
Sentinel Events
Sentinel events are a subcategory of adverse events. These events are unexpected and result in death, severe permanent or temporary physical or psychological harm to a patient, or the risk thereof (any process variation for which a reoccurrence would carry a significant risk of a serious adverse outcome); once discovered, sentinel events require immediate investigation into the cause and require health care organizations to develop corrective measures. These events also include injuries occurring due to deviation from policy or expected practice. A sentinel event is unrelated to the patient’s medical history and underlying conditions (TJC, 2025b; Patel & Goldin, 2025; Rodziewicz et al., 2024). The following are considered sentinel events:
- the suicide of any patient receiving care or within 72 hours of discharge from the hospital, including the emergency department (ED)
- the unanticipated death of a full-term infant
- an infant who is discharged with the wrong family
- the abduction of any patient who is receiving care, treatment, or services
- the unauthorized departure of a patient from a continuously staffed facility, including an ED, that leads to death, temporary harm, or permanent harm
- the administration of blood or blood products that have ABO and non-ABO incompatibilities, hemolytic transfusion reactions, or transfusions resulting in temporary or permanent harm, or death
- the rape, assault, or homicide of any patient who is receiving care, treatment, or services while in a hospital or clinical setting
- a WSPE during surgery or an invasive procedure
- the unintended retention of a foreign object (URFO) after an invasive procedure or surgery
- a case of severe neonatal hyperbilirubinemia (bilirubin level greater than 30 mg/dL)
- the prolonged use of fluoroscopy, which results in tissue damage when evidence-based practice guidelines are not followed
- radiotherapy to the wrong body region, the wrong patient, or at a dose that is more than 25% higher than intended
- the presence of fire, flame, or unintended smoke, heat, or flashes during direct patient care caused by equipment operated or used by the hospital and in use during the time of the event, whether the staff is present or not
- an intrapartum maternal death
- an instance of severe maternal morbidity that reaches a patient and results in permanent harm or severe, temporary harm (TJC, 2025b; Patel & Goldin, 2025; Rodziewicz et al., 2024)
These examples are serious patient safety issues and signal the organization’s need for immediate response to protect patient safety. Sentinel events can be related to patient acuity, staff dependence on medical technology, pressure to reduce lengths of stay, and a shortage of nurses or other health care workers. Hospitals frequently find that the leading cause of sentinel events is a breakdown in communication across disciplines regarding a patient’s care plan. Most sentinel events result from a systems-related problem with several root causes, not from a single individual’s mistake . The TJC requires all accredited hospitals to define sentinel events for their institution. The definition is expected to be communicated to all departments within the facility and services associated with the institution. When a sentinel event is identified, the hospital is expected to respond by stabilizing the patient, communicating with the patient and family concerning the event, notifying the hospital leadership, investigating the incident, completing and submitting an RCA, developing a corrective action plan with a timeline for implementation, and showing improvement (TJC, 2025b; Patel & Goldin, 2025; Rodziewicz et al., 2024).
Root Cause Analysis
An RCA analyzes medical errors to identify safety improvement measures accurately. The root cause is a problem or factor that, when eliminated in a sequence of problems or faults, prevents the adverse event from occurring. The root cause is often different from the factor identified upon initial investigation. Since 1997, TJC has mandated that sentinel events be analyzed using RCA. When an event occurs, the organization has 45 days to submit an RCA and action plan outlining how the organization will implement changes to prevent the same error from happening again. If the institution fails to complete this step, it is placed on an accreditation watch. Being placed on this watch indicates that a sentinel event occurred at the facility. However, they still need to develop an acceptable action plan to ensure that the same error is not repeated. This process typically begins within 72 hours of the event. TJC publishes a Framework for RCA and an Action Plan for health care organizations to provide an example of a comprehensive, systematic analysis. The framework outlines the steps and information needed in an RCA for effective quality improvement (TJC, 2020; Patel & Goldin, 2025; Patra & De Jesus, 2023; Rodziewicz et al., 2024).
In 2015, the renamed Root Cause Analyses and Actions (RCA2) was introduced to improve the effectiveness of the original tool with a focus on preventing future harm. This was also the beginning of a standardized process for reporting events. The focus of the RCA2 review is to determine system vulnerabilities and the factors that resulted in the adverse outcome so they can be mitigated and ultimately eliminated. An RCA2 focuses on the underlying cause of an event and not the individual. There are sequential steps in an RCA2 that the organization must follow. These includes identifying which team members will participate in completing the RCA. Then all relevant information must be gathered from the individuals involved in the event, including patients and family members when applicable. Once all the information is collected, the team organizes it, leading to the identification of the root cause. Once this is determined, the team creates an action plan that the organization will implement to prevent the error from reoccurring. Once complete, the report is forwarded to TJC for review (TJC, n.d.-a; Patra & De Jesus, 2023).
There may be multiple root causes for an event or a problem, and all possible solutions must be identified to prevent future events at the lowest possible cost and in the simplest possible way. The RCA2 should determine a sequence of events or a timeline to understand the relationships between the root cause(s) and the event to prevent it from happening in the future. The process is designed to reduce the frequency of undesirable events that occur over time within the environment where the RCA2 is used. RCA2 is based on the five “whys” or the Five Rules of Causation (asking why five times to get to the real root of a problem). Asking these whys will lead to statements that describe the cause, effect, and event. For example, something (cause) leads to something (effect), which increases the likelihood that the adverse effect of something (event) will occur. To reduce the incidence of medical errors, their causes must be correctly identified, and plans must be developed to improve processes that reduce the risk, along with methods to measure the successes and failures of interventions. The stronger the corrective action is, the more likely the change will be effective and sustained over an extended period. Strong corrective actions do not rely on human factors for adherence. Examples include scanning barcodes before medication administration, implementing hard stops within the electronic medical record, and standardizing equipment across care settings. In contrast, examples of weak corrective action are staff education and training (National Patient Safety Foundation, 2015; Patra & De Jesus, 2023).
National Patient Safety Goals and a Culture of Safety
TJCs National Patient Safety Goals (NPSGs) were designed to improve patient safety by focusing on specific problems related to health care safety and how to solve them. The TJC reviews the NPSGs yearly as data is collected regarding emerging patient safety concerns. The goals are tailored to address the most urgent safety problems across health care each year. Current NPSGs can be accessed via the TJC website. There are separate chapters with individualized goals for each practice setting for HCPs to follow. There is an overlap between the safety goals of each chapter, but the goals are specific to the particular practice area (TJC, 2026a, 2026b). The different chapters addressed in the 2026 NPSGs include the following:
- Ambulatory Healthcare Chapter
- Assisted Living Community Chapter
- Behavioral Healthcare and Human Services Chapter
- Critical Access Hospital Chapter
- Home Care Chapter
- Hospital Chapter
- Laboratory Chapter
- Nursing Care Center Chapter
- Office-Based Surgery Chapter
- Rural Health Clinic Chapter
- Telehealth Chapter (TJC, 2026a, 2026b)
Effective January 1, 2026, TJC released the NPG chapter for hospitals and critical access hospitals. The NPG chapter replaces the former NPSG chapter and brings a sharper focus to key issues in health care. The chapter identifies existing TJC requirements and organizes them into 14 measurable topics with clearly defined goals (TJC, 2026b). The NPGs that apply to the hospital setting are listed in Table 3.
Table 3
2026 Hospital NPGs
Goal 1 Ensure that the correct patient receives the correct care at the correct time. | NPG.01.01.01 The hospital has a process in place to correctly identify patients when providing treatment, care, and services. NPG.01.02.01 The hospital reports critical results of tests and diagnostic procedures on a timely basis. NPG.01.03.01 The hospital manages the flow of patients throughout the hospital. NPG.01.04.01 The hospital has a process for handoff communication. NPG.01.05.01 The hospital improves the safety of clinical alarm systems. NPG.01.05.02 The hospital recognizes and responds to changes in a patient’s condition. NPG.01.05.03 Resuscitative services are available throughout the hospital. NPG.01.05.04 The hospital develops and implements processes for postresuscitation care. NPG.01.05.05 The hospital reviews resuscitation cases to identify opportunities for improvement. NPG.01.06.01 The hospital conducts a preprocedure verification process. NPG.01.06.02 The hospital marks the procedure site. NGP.01.06.03 The hospital performs a time-out before the procedure. |
Goal 2 The governing body and leadership team foster a culture of safety. | NPG.02.01.01 The mission, vision, and goals guide the hospital’s actions. NPG.02.02.01 The hospital addressed conflicts of interest and ethics. NPG.02.03.01 The hospital’s leaders design work processes to focus individuals on safety and quality issues. NPG.02.04.01 The hospital has a workplace violence prevention program. |
Goal 3 The hospital has an emergency management program. | NPG.03.01.01 Hospital leaders provide oversight and support of the emergency management program. NPG.03.02.01 The hospital develops an emergency operations plan based on an all-hazards approach. NPG.03.02.02 The hospital has a communication plan that addresses how it will initiate and maintain communications during an emergency. NPG.03.02.03 The hospital has a staffing plan for managing all staff and volunteers during an emergency or disaster incident. NPG.03.02.04 The hospital has a plan for providing patient care and clinical support during an emergency or disaster incident. NPG.03.02.05 The hospital has a plan for safety and security measures to take during an emergency or disaster incident. NPG.03.02.06 The hospital has a plan for managing resources and assets during an emergency or disaster incident. NPG.03.03.01 The hospital has a disaster recovery plan. NPG.03.04.01 The hospital has an emergency management education and training program. NPG.03.05.01 The hospital plans and conducts exercises to test its emergency operations plan and response procedures. NPG.03.06.01 The hospital evaluates its emergency management program, emergency operations plan, and continuity of operations plans. |
Goal 4 The hospital prioritizes excellent health outcomes for all. | NPG.04.01.01 Improving health outcomes for all the hospital’s patients is a quality and safety priority. |
Goal 5 The hospital prioritizes infection prevention and control. | NPG.05.01.01 The hospital implements its infection prevention and control program through surveillance, prevention, and control activities. NPG.05.02.01 The hospital implements processes to support preparedness for high-consequence infectious diseases or special pathogens. NPG.05.03.01 The hospital complies with either the current CDC or the current World Health Organization (WHO) hand hygiene guidelines. |
Goal 6 The hospital prioritizes pain management and safe prescribing practices. | NPG.06.01.01 Pain assessment and pain management, including safe opioid prescribing, are identified as an organizational priority. NPG.06.02.01 The hospital assesses and manages the patient’s pain and minimizes the risks associated with treatment. NPG.06.03.01 The hospital collects data on pain assessment and management. |
Goal 7 The hospital respects the patient’s right to safe, informed care. | NPG.07.01.01 The hospital respects the patient’s right to receive information in a manner the patient understands. NPG.07.02.01 The hospital honors the patient’s right to give or withhold informed consent. NPG.07.03.01 The hospital assesses the patient who may be a victim of possible abuse, neglect, and exploitation. NPG.07.04.01 The hospital treats the patient in a dignified and respectful manner. |
Goal 8 The hospital reduces the risk of suicide. | NPG.08.01.01 The hospital reduces the risk of suicide. |
Goal 9 The hospital develops and implements safe transplant practices. | NPG.09.01.01 The hospital uses standardized procedures for managing tissues. NPG.09.02.01 The hospital traces all tissue bi-directionally. NPG.09.03.01 The hospital investigates adverse events related to tissue use or donor infections. |
Goal 10 The hospital performs waived testing safely and consistently. | NPG.10.01.01 Policies and procedures for waived tests are established, current, approved, and readily available. NPG.10.02.01 Staff performing waived tests are competent. |
Goal 11 The hospital maintains workplace and patient safety. | NGP.11.01.01 The hospital manages security risks. NGP.11.02.01 The hospital assesses and manages the patient’s risk for falls. NPG.11.03.01 The hospital manages utility systems. |
Goal 12 The hospital is staffed to meet the needs of the patients it serves, and staff are competent to provide safe, quality care. | NPG.12.01.01 The hospital’s leadership team ensures that there is qualified ancillary staff required to meet the needs of the population served and determines how staff function within the organization. NPG.12.02.01 The nurse executive directs the implementation of a nurse staffing plan. NPG.12.03.01 For psychiatric hospitals that use Joint Commission accreditation for deemed status purposes: The psychiatric hospital develops and implements staffing plans according to law and regulation. NPG.12.04.01 The hospital verifies that staff complete all requirements for employment and practice within their scope of practice. NPG.12.05.01 The hospital provides education and training and evaluates staff competence. NPG.12.06.01 The hospital evaluates staffing during performance improvement activities. |
Goal 13 The hospital safely performs imaging services. | NPG.13.01.01 The hospital defines and verifies qualifications and education requirements for imaging services staff. NPG.13.02.01 The hospital’s imaging services have a designated leader and follow current safe imaging practices. NPG.13.03.01 The hospital manages imaging safety risks. NPG.13.04.01 The hospital monitors quality improvement projects related to imaging safety. |
Goal 14 The hospital has a medication management program that focuses on safety. | NPG.14.01.01 The hospital safely manages pharmaceutical services. NPG.14.02.01 The hospital selects and procures medications. NPG.14.03.01 The hospital labels all medications, medication containers, and other solutions on and off the sterile field in perioperative and other procedural settings. NPG.14.04.01 The hospital reduces the likelihood of patient harm associated with the use of anticoagulation therapy. NPG.14.05.01 The hospital maintains and communicates accurate patient medication information. NPG.14.06.01 The hospital has an active antibiotic stewardship program. |
(TJC, 2026c)
Culture of Safety
Fostering a culture of safety is vital to a safe environment for staff and patients. This concept originated outside health care in other fields dealing with complex and hazardous situations (e.g., air traffic control). Organizations that have minimized adverse events despite engaging in this type of work are known as high-reliability organizations. These organizations maintain a safe environment for all their employees, from management to frontline staff (AHRQ PSN, 2024b). The AHRQ defines a culture of safety as encompassing the following key features:
- recognition that a health care organization is high-risk and must consistently operate in a safe manner
- a blame-free environment where everyone is free to report errors and near misses without the fear of punishment or reprimand
- collaboration and encouragement of all disciplines to seek solutions for patient safety concerns
- an organizational commitment to allocate resources to address safety concerns (AHRQ PSN, 2024b)
A blame-free environment to identify areas of concern that may contribute to patient safety is crucial to ensuring providers at all levels understand the organizational commitment to establishing a safety culture. If a culture of “low expectations” prevails, poor teamwork and communication can lead to an underdeveloped safety culture. The institution’s culture can be evaluated through surveys such as the AHRQ’s Patient Safety Cultures Survey or the Safety Attitudes Questionnaire. These surveys ask HCPs to rate their current culture of safety within individual units as well as the overall organization. When an organization is found to have a poor culture of safety based on the surveys, specific measures can be taken to improve. However, sustained improvements can be challenging to achieve (AHRQ PSN, 2024b). The following measures are associated with improvements:
- teamwork training
- executive walking rounds
- unit-based safety teams
- rapid-response teams
- structured communication tools, such as situation, background, assessment, recommendation (SBAR; AHRQ PSN, 2024b)
When a culture of safety is centered on the ability to report errors and near misses, the complete removal of blame or accountability is difficult. Some errors require accountability; thus, a newer term, just culture, is often used instead. A just culture still focuses on the systemic problems that lead to errors; however, there is accountability for an individual when they engage in reckless behavior, such as ignoring policies, skipping safety steps, or not following the plan of care (Murray et al., 2022; Robichaux & Vittone, 2023). There are three types of individual behaviors within a just culture:
- human error, such as forgetfulness or a lapse in judgment
- at-risk behavior, such as behavior that increases risk but the risk is not recognized or mistakenly believed to be justified
- reckless behavior, such as making a conscious decision to disregard established standards (Murray et al., 2022; Robichaux & Vittone, 2023)
A just culture is characterized by demanding accountability and quality through improved processes and systems within the workplace. This promotes reporting errors or near misses that occur even when all preventive measures are followed, as employees should feel safe and supported. A just culture facilitates learning from mistakes and improving to prevent repeat errors (Murray et al., 2022; Robichaux & Vittone, 2023).
The Partnership for Patients Campaign
In 2011, the Centers for Medicare and Medicaid Services (CMS) Innovation Center initiated the Partnership for Patients (PfP) campaign, which focused on significant patient concerns and areas of harm. The campaign originated from patient safety concerns that began with the IOM’s 2000 report, with the goal of incorporating best practices that will enhance patient safety in all US hospitals. The focus of PfP is to reduce the rate of preventable hospital-acquired conditions (HACs) and 30-day readmissions (CMS, n.d., 2024). Examples of HACs addressed by PfP include:
- adverse drug events (ADEs)
- catheter-associated urinary tract infections (CAUTIs)
- central line-associated bloodstream infections (CLABSIs)
- fall and immobility injuries
- perinatal/obstetrical complications
- pressure injuries
- surgical site infections (SSIs)
- venous thromboembolisms (VTEs)
- ventilator-associated pneumonia (VAP; CMS, n.d., 2024)
The campaign aims to save lives, decrease harm, and reduce costs for CMS programs. It has successfully led to an estimated 20,500 fewer hospital deaths and up to $7.7 billion in health care dollars saved from the resulting reduction of HACs. This accounted for a reduction in HACs by 910,000 or 13%. The 30-day readmission rate of patients following discharge has also decreased by 20% (CMS, n.d., 2024).
Medication Errors
Medication errors are a leading cause of avoidable harm in health care. Medication errors occur in both inpatient and outpatient care settings. The NCCMERP (n.d.) defines a medication error as:
any preventable event that may cause or lead to inappropriate medication use or patient harm while the medication is in the control of the HCP, patient, or consumer. Such events may be related to professional practice, healthcare products, procedures, and systems, including prescribing, order communication, product labeling, packaging, and nomenclature, compounding, dispensing, distribution, administration, education, monitoring, and use. (para. 1)
Medication errors can increase the length of a hospital stay, the rates of hospitalizations and emergency room visits, the cost of care, and morbidity and mortality rates. Many medication errors occur during a transition of care. During hospitalization, an individual’s medication regimen is often changed or adjusted, including the medications used, their dosage, or their frequency. Poor communication, a lack of patient education and understanding, poorly written discharge instructions, and a hurried discharge process can increase the risk of medication errors. Although electronic prescriptions can be more convenient, the lack of a tangible (i.e., paper) prescription may indicate to some patients that they do not have any new medication orders. An estimated 53% of adults and older adults experience a medication error or medication discrepancy following discharge from the hospital (Alqenae et al., 2020; Rasool et al., 2020; WHO, n.d.).
A medication error may lead to an ADE. The AHRQ PSN (2024e) defines an ADE as “harm experienced by a patient as the result of exposure to a medication” (para. 1). Not all ADEs are related to an error. Preventable ADEs harm the patient (to any degree) and could have been avoided. About half of ADEs are preventable with proper caution. Ameliorable ADEs result in patient harm and may have been mitigated with the proper steps in place, although not completely avoidable. Finally, there are nonpreventable ADEs that patients may experience even with appropriate prescribing and administration. These are commonly known as an ADR or side effect and are not secondary to error. ADRs can be categorized as allergic (a hypersensitivity reaction that is immune-mediated and require prior exposure), dose-related (or intolerance/sensitivity; these are often predictable and may be avoided with start-low-and-go-slow dosing initiation or may be addressed by decreasing the dosage), idiosyncratic (these are unexpected or unexplained and are not dose-related), and side effects (these are generally expected and do not require intervention/are often self-limiting). Some ADRs/side effects are utilized to their advantage, despite not being the intended therapeutic effect of a drug (the use of an antihistamine such as diphenhydramine [Benadryl] in an OTC sleep aid to induce drowsiness). ADRs are a subtype of ADE and can be graded as mild, moderate, severe, or lethal. ADEs that do not result in harm to a patient are called potential ADEs (e.g., a near miss or close call; AHRQ PSN, 2024e; Lynch, 2025a).
ADEs are one of the most common types of inpatient medical errors. Globally, medication errors account for $42 billion in annual health care spending. This number does not include the cost of lost wages or productivity due to medication errors. Worldwide, medication errors account for 5–41.3% of all hospital admissions and 22% of readmissions following discharge from the hospital. This broad range of hospital admissions attributed to medication errors is due to the various methods for classifying medication errors and prescribing practices. Many outpatient medication errors are due to prescribing an unnecessary drug, a nonoptimal drug, or a nonoptimal dose. In the United States, medication errors affect over 7 million patients a year. Approximately 500,000 medication errors occur daily, resulting in 7,000–9,000 deaths annually. In the United States, more people die due to medication errors than to motor vehicle accidents, breast cancer, or autoimmune disorders. Approximately $40 billion is spent annually in the United States on patients affected by medication errors. Due to inconsistencies in reporting, the prevalence of medication errors varies based on the source (Naseralallah et al., 2025; Rasool et al., 2020; Tariq et al., 2024; WHO, n.d.).
Health care practitioners have access to over 10,000 prescription medications to offer patients as part of their treatment plan, and more than one-third of American adults take five or more medications daily. Even if the medications are taken precisely as ordered, there is ample opportunity for poor outcomes. There are specific patient, drug, and clinician risk factors for ADEs. Those most at risk are individuals who take more than five medications (polypharmacy), have multiple comorbidities, have a chronic illness, consult numerous providers, are over 65, and have limited health literacy. The risk of experiencing a medication error when taking five or more prescription medications is 30%. Individuals over 75 have a 38% chance of experiencing a medication error. Patients with developmental delays, mental health conditions, language barriers, cognitive impairments, decreased level of consciousness, and sensory disturbances are also at an increased risk of experiencing a medication error. Pediatric patients also have a higher risk for ADEs and should be dosed according to weight rather than age. Since older adult and pediatric populations are at increased risk for ADEs, nurses should be careful when administering medications to these populations and ensure that patient education has been given, reinforced, and understood by patients and caregivers before discharge from the acute care setting. Other patient-specific risks lie with health literacy and the ability to use basic math operations for daily tasks. In the community setting, parents, patients, and caregivers often cause ADEs due to misunderstanding the directions for administration (AHRQ PSN, 2024e; Harris, 2024; Rasool et al., 2020; Tariq et al., 2024).
There are two major types of errors: errors of omission and errors of commission. An example of an error of commission would be administering amoxicillin (Amoxil) to a patient with a penicillin (PCN) allergy. Medication errors can occur at any stage of the medication use process. TJC, WHO, and NCCMERP divide medication errors into different taxonomies based on the source of the error (e.g., improper storage leading to the deterioration or contamination of the drug). Errors can also occur during the prescribing phase or the utilization stage. These includes errors that arise during dispensing, administration, and monitoring stages. Medication errors are frequently the result of system failures and human error (Rodziewicz et al., 2024; Tariq et al., 2024). The most common system errors are:
- incorrect order transcription
- failure to verify orders completely
- poor dissemination of medication education
- neglecting to verify patient allergy information or history
- a lack of interdisciplinary communication (AHRG PSN, 2024e; Lynch, 2025b; Tariq et al., 2024)
Human error often results from fatigue, poor communication or hand-off, and inadequate staffing. The most common human mistakes that cause medication errors include:
- failure to communicate orders
- illegible handwriting
- wrong drug selection when ordering electronically
- confusing similarly named drugs
- choosing the wrong medication when packaged similarly
- selecting the wrong dose
- administering the medication via the wrong route, at the wrong time, to the wrong patient, or at the incorrect infusion rate or dose
- administering an additional dose or omitting a dose
- not following established protocols or utilizing workarounds (AHRQ PSN, 2021; Tariq et al., 2024; WHO, n.d.)
Medication errors can also be categorized based on whether they are rule-based, memory-based, knowledge-based, or action-based (Ambwani et al., 2019; Ottosen & Bucknall, 2024):
- Rule-based errors occur when nurses use a bad rule or misapply a good one. An example of a failure to apply a good rule is a nurse who hangs a bag of total parenteral nutrition (TPN) without cross-checking the ingredients with the current provider’s order or asking a second nurse to perform a double-check. The application of a bad rule might be a facility that does not have an established policy requiring double-checks of TPN before patient administration. Either situation could result in a poor patient outcome. These errors can be avoided through proper training and education and consistent implementation of existing rules (e.g., policies and procedures).
- Memory-based errors occur due to memory lapses. An example is a nurse who administers PCN (Pen-Vee K) to a patient they know has an allergy to PCN but forgets. These errors can be avoided with computerized prescribing systems and cross-checking allergies with each medication administration.
- Knowledge-based errors occur when nurses are missing information. An example is administering PCN (Pen-Vee K) to a patient without first establishing whether they have an allergy. These errors can be avoided through appropriate information intake on admission and computerized prescribing systems that track patient information so that pharmacists, providers, and nurses can cross-check each other.
- Action-based errors are primarily due to carelessness while routinely prescribing, dispensing, or administering medications. Examples include a pharmacist adding the wrong amount of potassium chloride into an intravenous (IV) bag due to distractions, a nurse who draws up 5 mL of a medication rather than 0.5 mL into a syringe because they were rushed while preparing the medication, or a nurse who overrides the electronic dispensing system to dispense a medication, believing it to be required, not realizing that the provider had discontinued it earlier. This type of error can be avoided by minimizing distractions, cross-checking orders with a second nurse, following the rights of medication administration, and using bar codes.
A list of high-risk medications that can cause significant patient harm if used in error was published by the Institute for Safe Medication Practices (ISMP). It includes medications with dangerous adverse effects, look-alike/sound-alike (LASA) names (refer to Table 4), or similar physical appearances but different pharmaceutical properties. The ISMP’s List of Confused Drug Names includes LASA drugs that nurses should know to avoid common opportunities for error. Some medications can cause severe harm when misused. These medications should have additional safeguards in place to protect patients from harm. One such safeguard requires two nurses to verify that the correct medication and dose are being administered to a patient (AHRQ PSN, 2024e; ISMP, 2024a, 2024b; Rodziewicz et al., 2024). Examples of high-risk medications include:
- adrenergic agonists (epinephrine [Adrenalin] subcutaneous [SQ] or intramuscular [IM], norepinephrine [Levophed])
- adrenergic antagonists (propranolol [Inderal], metoprolol [Lopressor], labetolol [Normodyne])
- epoprostenol sodium (Flolan) IV
- antiarrhythmics IV (lidocaine [Xylocaine], amiodarone [Cordarone])
- vasopressin (Pitressin) IV or intrasseous (IO)
- insulin (all formulations and routes of administration, especially U-500)
- antithrombotic agents
- anticoagulants (warfarin [Coumadin], low molecular weight heparin [Fragmin, Lovenox], unfractionated heparin)
- direct oral anticoagulants and factor Xa inhibitors (rivaroxaban [Xarelto], fondaparinux [Arixtra])
- direct thrombin inhibitors (argatroban [Acova], bivalirudin [Angiomax], dabigatran [Pradaxa])
- glycoprotein IIb/IIIa inhibitors (eptifibatide [Integrilin])
- thrombolytics (alteplase [Activase], reteplase [Retavase], tenecteplase [TNKase])
- magnesium sulfate IV
- cardioplegic solutions
- chemotherapeutic agents (parenteral and oral)
- dextrose, hypertonic, 20% or greater
- dialysis solutions (peritoneal and hemodialysis)
- epidural and intrathecal medications
- methotrexate (Rheumotrex) oral for nononcologic use
- liposomal forms of medications
- minimal and moderate sedation agent, oral, for children (midazolam [Versed])
- moderate sedation agents, IV (dexmedetomidine [Precedex], midazolam [Versed], lorazepam [Ativan])
- nitroprusside sodium (Nipride, Nitropress) IV
- neuromuscular blocking agents (succinylcholine [Anectine], rocuronium [Zemuron], vecuronium [Norcuron)
- potassium chloride concentrate IV
- potassium phosphates IV
- promethazine (Phenergan) IV
- oxytocin (Pitocin) IV
- benzodiazepines
- tranexamic acid (Lysteda) IV
- opium tincture
- opioids, all routes of administration
- parenteral nutrition preparations
- sodium chloride IV, hypertonic, greater than 0.9% concentration
- sterile water infection in containers of 100 mL or more
- sulfonylurea hypoglycemics, oral (glimepiride [Amaryl], glipizide [Glucotrol], glyburide [DiaBeta])
- anesthetics (propofol [Diprivan], ketamine [Ketalar]; ISMP, 2024b; Rodziewicz et al., 2024)
Table 4
LASA Medications
Drug | LASA |
Alprazolam | Clonazepam |
Amiodarone | Amantadine |
Asacol | Os-Cal |
Benadryl | Benazepril |
Buspirone | Bupropion |
Celexa | Zyprexa |
Clonidine | Klonopin |
Desmopressin | Vasopressin |
Diazepam | Diltiazem |
Dopamine | Dobutamine |
Epinephrine | Ephedrine |
Fluoxetine | Duloxetine |
Glyburide | Glipizide |
Inderal | Adderall |
Lunesta | Neulasta |
MiraLAX | Mirapex |
Patanol | Platinol |
Prednisone | Prednisolone |
Prenexa | Ranexa |
Prozac | Prograf |
Ribavirin | Riboflavin |
Rifampin | Rifaximin |
Sertraline | Cetirizine |
Sitagliptin | Saxagliptin |
Zantac | Zyrtec |
Zebeta | Diabeta |
Zyban | Diovan |
(ISMP, 2024a)
Nurses can avoid medication errors by using the rights of medication administration, a systematic approach designed to recognize errors before they reach a patient during medication administration. CMS has identified five fundamental rights of medication administration. Other sources refer to any number from five to ten rights of medication administration (CMS, 2020; Hanson & Haddad, 2023; Wisconsin Technical College System, 2023). The National Council of State Boards of Nursing (2023) test plan notes that the rights of medication administration should be followed when giving medications; however, it does not elaborate any further regarding the number of medication rights.
The 10 possible rights of medication administration consist of the following (CMS, 2020; Hanson & Haddad, 2023; Henshaw & Rassilyer-Bomers, 2023; Wisconsin Technical College System, 2023):
Right patient: This information should be verified by the patient or patient wristband using two separate patient identifiers, including the patient’s name, medical record number, or date of birth; the nurse must verify that this information matches the medication label (if applicable) and medication administration record (MAR).
Right drug: The medication being given must match the order in the MAR; the nurse must also verify that the patient does not have an allergy to the medication.
Right dose: the nurse must verify that the dose being given matches the order and is appropriate for the patient.
Right route: The nurse must verify that the medication can be administered via the route ordered and that the route ordered is appropriate for the patient (e.g., medications should not be given orally if the patient is unable to take anything by mouth).
Right time or frequency: The nurse must ensure that the prescribed frequency or scheduled time of administration is being followed; this is especially true for medications that must be administered at a specific time (e.g., antibiotics) or for as-needed medications that are not scheduled to ensure they are not given too frequently.
Right education: Information should be provided to the patient about the drug being administered, including the indication for use and potential adverse effects.
Right documentation: Proper documentation must be completed to indicate that the medication has been given, preventing a possible duplicate dose.
Right history and assessment: The nurse should review the patient’s allergies (if not done during the right drug check) and any history of medication reactions; the patient’s history should also be checked for possible drug interactions. This step also includes collecting any assessment data necessary before administering a medication. For example, checking a blood pressure before administering an antihypertensive medication.
Right to refuse: After the patient is informed about the medication, they have the right to refuse administration; this must be documented and communicated to the prescribing provider.
Right evaluation: The nurse should monitor the patient and evaluate them for potential adverse effects.
The medication administration rights should be performed methodically in a process known as the three checks. The three checks should be performed systematically to make the process a habit (Henshaw & Rassilyer-Bomers, 2023; Wisconsin Technical College System, 2023). The rights of medication administration should be completed in the following order:
- First check: as the medication is removed from the dispensing machine or medication cart
- Second check: before being removed from a multidose container; if required per facility policy, this is when a second nurse performs their safety check
- Third check: this happens at the patient’s bedside before administering the medication to the patient (Henshaw & Rassilyer-Bomers, 2023; Wisconsin Technical College System, 2023)
In addition to the ten rights and three checks, nurses should ensure that hand-offs are thorough and that essential information has been communicated to the oncoming or receiving nurse. Bar-code-scanning technology, electronic health records, and computerized prescriber order entry can reduce medication errors when appropriately used (AHRQ PSN, 2024e; Tariq et al., 2024).
Goal 14 of the NPGs addresses medication management programs that focus on safety. Six performance measures in the 2026 NPGs include (1) safely managing pharmaceutical services, (2) selecting and procuring medications, (3) labeling all medications, containers, and solutions, (4) reducing the likelihood of patient harm associated with anticoagulant therapy, (5) maintaining and communicating accurate patient medication information, and (6) having an active antibiotic stewardship program. How medications are labeled and packaged can lead to medication errors, especially when drugs are removed from their original container and placed into an unlabeled container (i.e., syringe or medication cup). This practice can cause harmful errors leading to death. Medications must be labeled with the medication name, strength, amount of medication if not evident from the container, diluent name if applicable, expiration date, and time if not being used immediately (Henshaw & Rassilyer-Bomers, 2023; TJC, 2026c).
Anticoagulation therapy is widely used for both treatment and prophylaxis of VTE, for treating atrial fibrillation and pulmonary embolism, and after a mechanical heart valve implant. However, anticoagulant use increases a patient’s risk of experiencing a medication error or harm from complex dosing, poor monitoring, and lack of compliance with the treatment. Hospitals should follow approved protocols based on evidence-based practice guidelines regarding the use of anticoagulants. These guidelines consider weight-based dosing, age adjustments, renal or liver function adjustments, and drug interactions. The guidelines also outline how the patient should be monitored and how often laboratory values should be checked. Not following these guidelines and hospital policy can lead to medication errors and poor patient outcomes (Amaraneni et al., 2024; Henshaw & Rassilyer-Bomers, 2023; TLC, 2026c).
Medication reconciliation is the process of creating an accurate list of all medications a patient takes to avoid errors. Medication reconciliation is designed to identify and resolve discrepancies on the medication list. The medication list must include the drug name, dosage, frequency, and route. To ensure the correct medications are administered, the medication list must be compared to the provider’s orders at the time of admission, when transferred between hospital units, and at discharge. Potential errors during medication reconciliation are omitting a medication, recording the medication more than once, or recording an incorrect dose/frequency (AHRQ PSN, 2024f; Institute for Healthcare Improvement, 2018; TJC, 2026c).
The prevention of medication errors is the responsibility of the entire health care team. A nurse’s obligations to prevent medication errors include the following:
- knowing federal, state (nurse practice acts), and local laws and facility policies that govern the prescribing, dispensing, and administration of medications
- performing accurate dosing calculations when indicated
- preparing, administering, and evaluating the patients’ responses to medications
- developing and maintaining up‑to‑date knowledge of medications administered commonly in the nurse’s practice area, including uses, mechanisms of action, routes of administration, safe dosage range, adverse reactions, side effects, precautions, contraindications, and interactions
- maintaining knowledge of acceptable practice and skill competencies
- determining the accuracy of medication orders
- reporting all medication errors
- safeguarding and storing medications per the manufacturer’s instructions (Burchum & Rosenthal, 2024; Tariq et al., 2024)
Any of these medication errors can lead to a sentinel event, causing a health care organization to implement an RCA to determine the cause(s). Figure 1 depicts an example of an RCA, such as the TJC Sentinel Event Alert #61 for the safety of oral anticoagulants. For more information on this topic, please refer to the NursingCE activity entitled Medication Errors.
Figure 1
RCA of a Medication Error
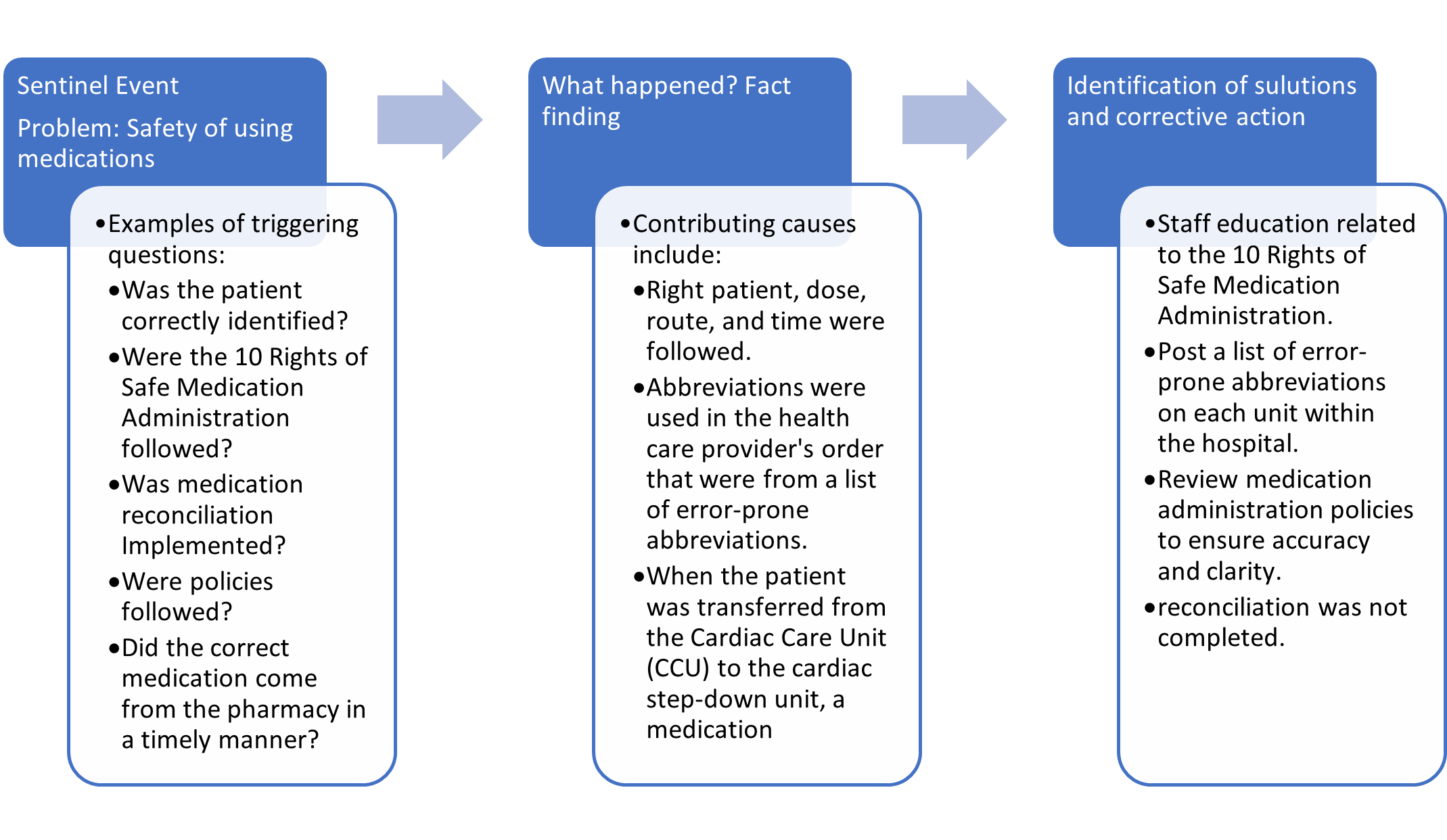 (adapted from TJC, 2019)
(adapted from TJC, 2019)
Hospital-Associated Infections
HAIs are nosocomial infections that manifest in a health care setting while the patient receives care for another condition. This terminology does not imply that an infection was caused solely by the health care services rendered but only that it manifested following admission to the health care facility. HCAIs can develop in any health care facility, including hospitals, ambulatory clinics, surgical centers, inpatient rehabilitation facilities, and long-term care settings. Since some references have stated that HCAI is a retired term and other sources refer to both categories of infection as hospital-acquired with the designated acronym “HAI,” this terminology is used throughout this learning module (CDC, 2025a; Monegro et al., 2023; National Healthcare Safety Network [NHSN], 2026a).
HAIs can be endogenous (developing from the patient’s flora) or exogenous (originating outside the patient’s body). Reservoirs known for causing exogenous HAIs include the hands of HCPs, other patients, equipment (e.g., blood pressure cuffs, urine collection devices), and the environment (e.g., contaminated surfaces, toilets, sinks, doorknobs). In the United States, HAIs affect about 1.7 million inpatients annually, leading to more than 270,000 deaths yearly. According to the CDC (2024), approximately 1 in 31 hospitalized patients and 1 in 43 residents of skilled nursing facilities (SNFs) report at least one HAI daily. HAIs are associated with high morbidity and mortality, with devastating impacts, including prolonged hospitalization, increased suffering, lost productivity, and substantial costs to the health care system and society. HAIs are monitored closely by agencies such as the NHSN, the most widely used HAI-tracking system. The NHSN collects data to identify problematic areas and standardize infection rates to measure, track, and evaluate HAI prevention modalities. This monitoring allows for a more accurate and direct comparison of infection rates between health care facilities and trends over time. Common HAIs include CLABSI, CAUTI, SSIs, hospital-acquired pneumonia (HAP), VAP, Clostridioides difficile (C. diff) infection, methicillin-resistant Staphylococcus aureus (MRSA) infection, and vancomycin-resistant enterococci (VRE) infection (CDC, 2024d; Monegro et al., 2023; NHSN, 2026a; Office of Disease Prevention and Health Promotion, n.d.).
The risk for HAIs depends on multiple influences, such as the infection prevention practices of the health care facility, the prevalence of pathogens within the community or health care setting, and individual patient factors (e.g., compromised immune system, increased length of stay, and comorbidities such as heart disease, chronic obstructive pulmonary disease [COPD], and DM). Bacteria are the most common cause of infections following surgery. SSIs account for 20% of all HAIs, costing approximately $3.3 billion. Bacteria can infect a surgical site through a contaminated caregiver, surgical instruments, or bacteria already on the patient’s body (CDC, 2024d; NHSN, 2026b). The CDC has identified three types of SSIs:
- superficial incisional infection, which occurs just in the area of the incision
- deep incisional infection, which occurs in the muscle and the tissues surrounding the muscle beneath the incision
- organ/space infection, which occurs in any area of the body, a body organ, or a space between organs (NHSN, 2026b)
Catheter-Associated Urinary Tract Infection
A urinary tract infection (UTI) involves any part of the urinary system, including the urethra, bladder, ureters, and kidneys. UTIs account for over 9.5% of all infections reported by acute care hospitals. According to the NHSN (2026a), 12–16% of hospitalized adults will have an indwelling urinary catheter at some point during their hospitalization. Indwelling urinary catheters contribute to 75% of health care–associated UTIs. A CAUTI is diagnosed based on a positive urine culture when an indwelling urinary catheter has been in place for more than 48 hours. CAUTIs can occur from unsterile catheterizations, repeated catheterizations, and improper drainage system management. Gram-negative bacilli are the primary bacteria that cause UTIs (American Nurses Association [ANA], n.d.-a; Imam, 2024; NHSN, 2026a).
The most effective strategies to prevent CAUTIs are to avoid using an indwelling urinary catheter and to remove an existing catheter as soon as possible. For patients with an indwelling catheter inserted before surgery, removing the catheter within 24 hours postoperatively is critical for prevention. Intermittent catheterization is preferable to an indwelling catheter whenever possible. Nurses must also utilize appropriate aseptic technique and sterile equipment for catheter insertion in the hospital environment. If breaks in aseptic technique, disconnection of the closed system, or leaks occur, the catheter and drainage bag should be replaced using aseptic technique and sterile supplies. A nurse-driven CAUTI prevention tool from the ANA features a decision-making tree based on the 2009 CDC criteria for inserting an indwelling urinary catheter to determine whether insertion is indicated (ANA, n.d.-a, n.d.-b; Imam, 2024).
According to evidence-based guidelines, the vital elements of nursing care to prevent infection center on the appropriate management of urinary catheters:
- insert an indwelling urinary catheter only when indicated
- remove the urinary catheter as soon as it is no longer indicated
- properly secure indwelling catheters after insertion
- maintain a sterile closed drainage system
- replace the catheter and drainage bag using aseptic technique
- obtain urine samples by aspirating urine from the sampling port using a sterile syringe
- maintain unobstructed urine flow
- always keep the urinary drainage bag below the level of the bladder; do not place the bag on the floor
- perform routine hygiene and do not use antiseptics to clean the periurethral area (ANA, n.d.-a, n.d.-b; Ignatavicius et al., 2023; Imam, 2024)
Central Line-Associated Bloodstream Infection
CLABIs are severe and potentially fatal bloodstream infections that can occur from a breach in sterile technique during the insertion procedure, improper or inadequate care or management of the line, and medication administration. Central lines provide direct access to the major vessels in the venous circulatory system and remain in situ for long periods. Since the catheter provides a portal of entry and a direct pathway to the venous system, an infectious agent can quickly spread throughout the bloodstream, generating critical and systemic illness. Bloodstream infections can induce hemodynamic changes, leading to organ dysfunction, sepsis, shock, and death. According to the NHSN (2026a), there has been a 10% decrease in CLABSIs across US hospitals between 2023 and 2024; however, more than 18,100 CLABSIs still occur in acute care facilities (including ICUs) each year. The estimated cost of each CLABSI case is around $46,000 and carries a mortality rate of 10–30% (CDC, 2017; Haddadin et al., 2022; Rahmani et al., 2022).
Since October 2008, CMS no longer reimburses for HAIs, including CLABSI. In addition, the CDC published revisions to their 2011 Intravascular Catheter-Related Infections Guidelines in 2017. In partnership with several accredited organizations, these guidelines determined the evidence-based practice (EBP) standards for preventing CLABSI and other HAIs. The CDC and the Infusion Nurses Society (INS) guidelines present consistent recommendations. Table 5 offers an overview of these critical aspects of vascular access device (VAD) care to prevent a CLABSI (CDC, 2017; Nickel et al., 2024).
Table 5
5 Core Components of VAD Care
Essential I
Hand hygiene using the correct technique | Hand hygiene should be performed using an alcohol-based rub in the following instances:
Hand hygiene should be performed using an antimicrobial soap and water instead of an alcohol rub when hands are visibly contaminated or soiled, after providing care or having direct contact with a patient who has norovirus or a spore-forming pathogen (e.g., C. diff infection), before eating, and after using the bathroom. |
Essential II
Maximal barrier precautions | Maximal barrier precautions should be used when inserting central lines. Central line insertion is a sterile procedure. The clinician inserting the line and those assisting should wear appropriate personal protective equipment (PPE), including a cap (covering all hair), a mask (covering the nose and mouth tightly), a sterile gown, and sterile gloves. A sterile drape should cover the patient from head to toe, and a sterile dressing should be applied immediately after insertion. |
Essential III
Chlorhexidine skin antisepsis | Chlorhexidine skin antisepsis should be performed before inserting a CVC and when changing the sterile dressing. The skin should be prepped with chlorhexidine 2% in 70% isopropyl alcohol. A single-use povidone-iodine or 70% alcohol application is recommended as an alternative for patients with sensitivity to chlorhexidine. The applicator sponge should be held against the skin to allow the antiseptic solution to saturate the pad. The insertion site should be scrubbed in a back-and-forth motion for at least 30 seconds. The antiseptic should air dry for maximal effect (about 2 minutes). Avoid wiping or blotting before puncturing the site or applying a new dressing. |
Essential IV
Optimal site selection | The optimal site should be selected using the smallest gauge catheter and the fewest lumens required for the prescribed or anticipated therapies. The subclavian vein may decrease the risk of infection compared to the jugular vein, and the subclavian vein is generally preferred for nontunneled catheters. The femoral vein should be avoided whenever possible due to higher risks of infection, bleeding, and thrombosis, especially for overweight adults. Other factors, such as HCP skill and the potential for mechanical complications or vein stenosis, should be considered. The rationale for the chosen site should be documented. |
Essential V
Daily assessment | The VAD must be assessed daily for continued necessity and the potential for prompt removal. The VAD should be removed as soon as it is no longer clinically indicated. Daily VAD assessment should include, at a minimum, the following components, which must be documented in a flowsheet in the patient’s medical record:
|
(CDC, 2017; DeVries, 2019; Haddadin et al., 2022; Jarding & Makic, 2021; Nickel et al., 2024)
Nursing care for patients at risk for CLABSIs includes hand hygiene and appropriate infection control precautions, such as disinfecting the catheter hub or injection port before accessing the line. To prevent CLABSIs and increase compliance, TJC implemented “Scrub the Hub!” to remind HCPs to disinfect the catheter hub before accessing the line. Antiseptic barrier caps have also been shown to decrease the risk of CLABSIs. These devices are in constant contact with the catheter hub and optimize disinfection without active scrubbing of the hub. All IV tubing should be changed per policy, usually within 24 hours for intermittent infusions and 96 hours for continuous infusions (excluding lines used for lipids or blood products). All ordered antibiotics should be administered as prescribed to ensure patients receive the proper treatment. Nurses also need to continue to monitor for signs that the CLABSI is resolving or worsening (CDC, 2017; Haddadin et al., 2022; TJC, n.d.-b; Nickel et al., 2024).
Prevention of HAIs
Proper hand hygiene is the most effective risk-reduction strategy to prevent HAIs. According to the CDC, HCPs wash their hands or perform hand hygiene less than 50% of the time that it is indicated. Performing hand hygiene in the presence of patients and their families promotes trust and models good behavior for others. “Hand hygiene” refers to handwashing with an antimicrobial or plain soap and water and alcohol-based products such as gels, foams, and rinses. Alcohol-based products contain an emollient that does not require the use of water. According to the CDC, in the absence of visibly soiled hands or when contamination from spore-forming organisms (e.g., C. diff) is unlikely, approved alcohol-based products for hand disinfection are preferred over antimicrobial or plain soap and water because of their superior microbicidal activity, reduced drying of the skin, and convenience in the absence of a sink (CDC, 2024a, 2024c).
HCPs are advised to inspect their hands for breaks, cuts, or lacerations in the skin or cuticles before the start of each workday. These open areas provide a portal of entry for organisms. If any breaks in skin integrity are identified, a dressing should be applied before caring for patients. Performing hand hygiene between tasks and procedures on the same patient may be necessary to prevent cross-contamination between different body sites. Artificial nails are discouraged since they harbor microorganisms. Fingernails should be trimmed to one-quarter of an inch, and rings should be avoided if possible. If the areas beneath the fingernails are soiled, they should be cleaned with an orangewood stick, if available (CDC, 2024a, 2024c).
Nurses should educate patients and family members on infection prevention techniques, such as:
- keeping all dressings clean, dry, and intact and reporting any concerns with the bandage, such as loosening around the edges or dislodgement
- reporting if the area around the IV catheter insertion site becomes red, warm, or sore or if they experience chills or other symptoms of a fever
- reinforcing the importance of maintaining a clean environment
- refraining from touching any lines or tubing
- enforcing that anyone entering the room must wash their hands when they enter and exit (Ignatavicius et al., 2023)
Any of these HAIs can lead to a sentinel event, causing the health care organization to implement an RCA to determine the cause(s). Figure 2 depicts an RCA identified by the TJC Sentinel Event Alert #28 for decreasing HAIs. For more information on this topic, please refer to the NursingCE activity entitled Hospital-acquired Infections.
Figure 2
RCA of an HAI
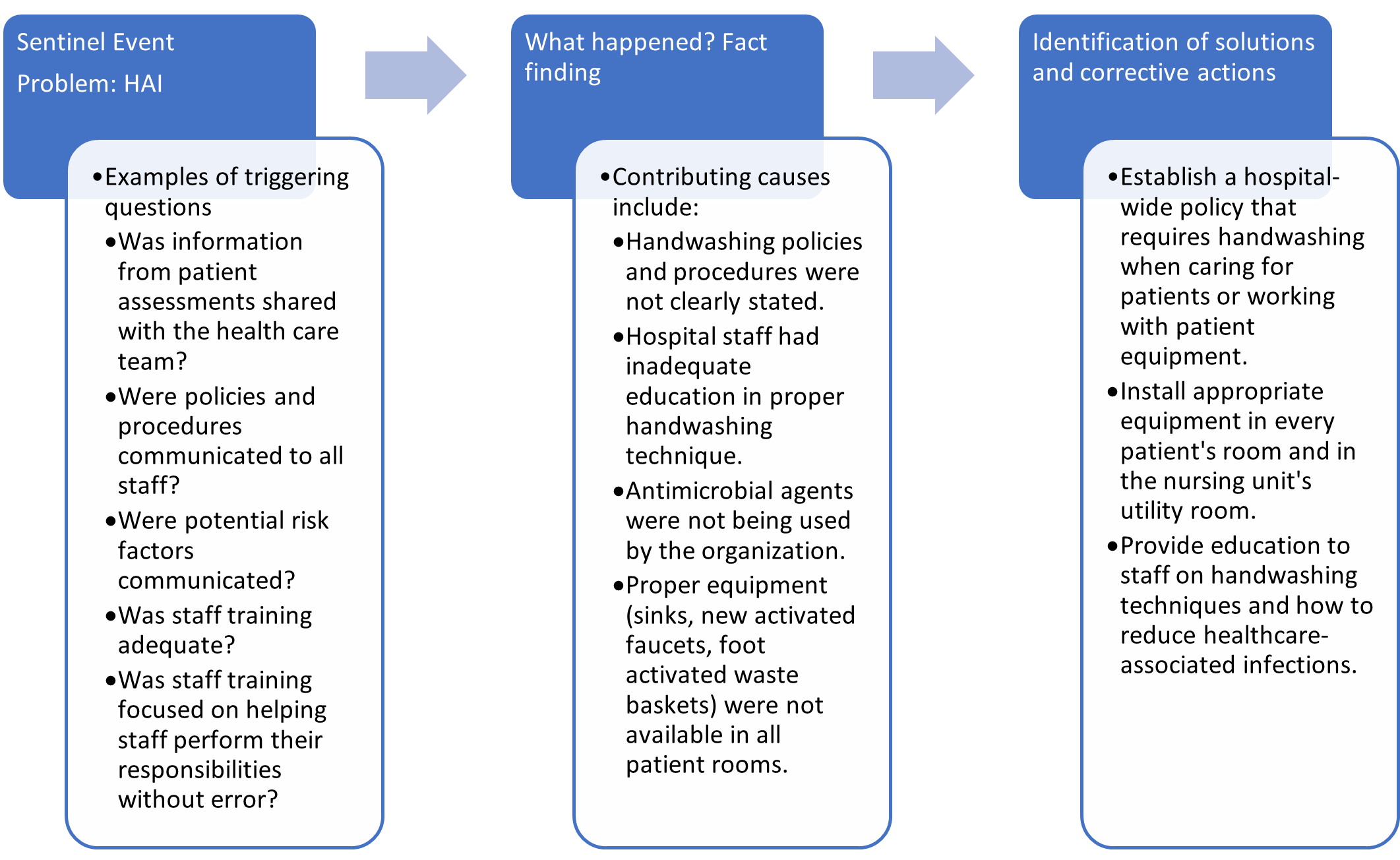
(adapted from TJC, 2003)
Injuries Related to Falls and Immobility
TJC includes fall reduction as a core performance measure (Goal 11) in the NPGs for 2026. Hospitals have devoted quality improvement and research efforts to prevent falls, but patient falls are continually the most common adverse event that occurs in hospitals. A fall is defined as any unplanned descent to the floor. Approximately 2% of patients admitted to the hospital will fall at least once, and 25% of these falls result in injury. In 2008, CMS stopped reimbursing hospitals for injuries that occurred as a direct result of a fall. Each year, approximately 700,000 to 1 million individuals fall. These falls result in 250,000 injuries and 11,000 deaths. Injuries range from bruises, soft tissue injuries, and fractures to severe traumatic brain injuries. The cost per patient for each injury ranges from $35,475 to $36,776, running into billions yearly for direct and indirect costs. Direct costs include hospital and nursing home fees, healthcare providers, therapists, nurses, medical equipment, and prescription drugs. Indirect costs are disability, loss of income, and poor quality of life (AHRQ PSN, 2024h; Gervasi et al., 2025; TJC, 2026c). Several factors can increase an individual’s risk of falling, including:
- weakness in the lower limbs
- vitamin deficiency, especially vitamin D
- gait disturbances
- use of certain medications, including sedatives, antidepressants, diuretics, and antihypertensives
- changes in vision
- presence of hazards in the home, including uneven elevation changes or loose rugs
- not utilizing the call light in the hospital
- age over 65 (CDC, 2024b; LeLaurin & Shorr, 2019; National Alliance for Caregiving [NAC], n.d.)
Individuals over age 65 are at an increased risk of falling due to changes that occur during aging. As humans age, there is a loss of coordination, flexibility, and balance, primarily through inactivity, making falling easier. In aging eyes, less light reaches the retina, making contrasting edges, tripping hazards, and obstacles harder to see. Polypharmacy in older adults is more common, and some medications can cause dizziness, dehydration, or interactions with each other, leading to a fall. Most older adults have lived in their homes for a long time and have never thought about simple modifications that might keep them safer. Over 90% of older adults have at least one chronic condition like DM, stroke, or arthritis. These often increase the risk of falling due to lost function, inactivity, depression, pain, or multiple medications (NAC, n.d.). Refer to Figure 3 for an RCA of falls.
Figure 3
RCA of Falls
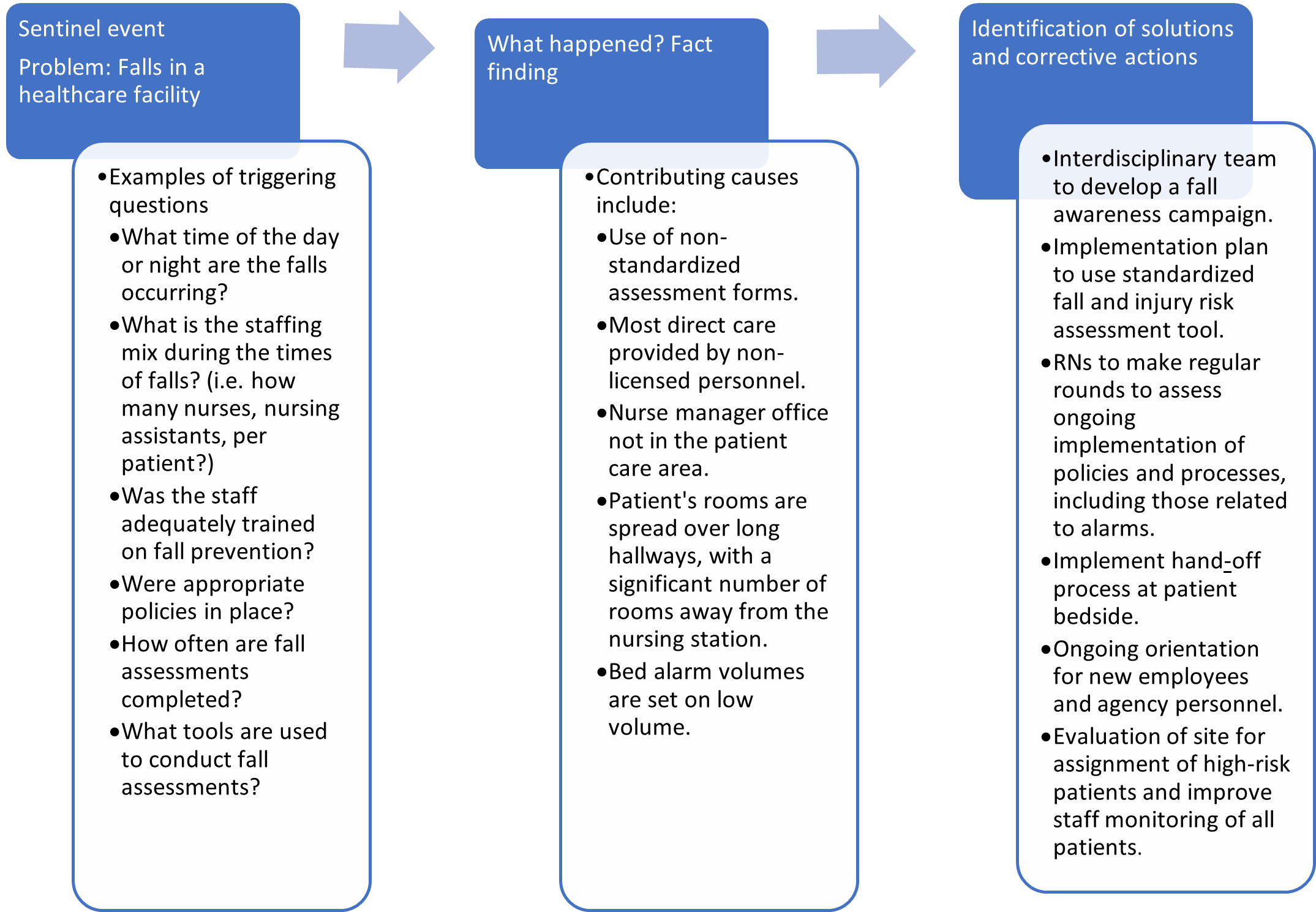 (adapted from TJC, 2015)
(adapted from TJC, 2015)
Fall Prevention
Behavioral and environmental changes can be made to prevent falls. Some of these preventive measures are known as universal fall precautions since they can be applied to anyone (AHRQ PSN, 2024h; Appeadu & Bordoni, 2023). Examples of preventive measures that can be implemented in patient care settings to decrease the risk of falling include:
- familiarize the patient with the environment if it is unfamiliar; reorient individuals who may be confused
- keep all necessary belongings within reach
- have handrails available in the bathroom and hallways
- if a hospital bed is present, keep the brakes locked and the bed in the lowest position
- when they are out of bed, encourage patients to wear nonslip, well-fitting footwear
- use night lights to help illuminate walkways
- keep floors uncluttered and dry
- implement extra precautions for those with cognitive deficits
- educate patients and their families on the use of call lights, the patient’s risk for falls, and not getting out of bed without assistance
- educate patients and their families on the side effects of their medications and, particularly, any increased risk of falls (AHRQ PSN, 2024h; Appeadu & Bordoni, 2023)
Targeted solutions are suggested for patients at increased risk for falls. For example, if a patient falls or is at risk of falling while toileting, the staff should perform hourly rounding to toilet the patient proactively and avoid unassisted ambulation. For medications that put a patient at risk of falls, there should be targeted education on the medication’s side effects and the increased risk of falling, along with scheduling the medication administration at least 2 hours before bedtime. Older adults should develop a fall prevention action plan with their family, including a review of their risk factors and a plan to minimize risk. Public education campaigns regarding reducing fall risks at home (e.g., throw rugs, clear lighting in pathways/walkways) may allow nurses to extend fall prevention efforts beyond the health care setting (AHRQ PSN, 2024h; Appeadu & Bordoni, 2023; NAC, n.d.).
Pressure Injuries
Pressure injuries are localized damaged skin and soft tissue areas caused by unrelieved pressure, friction, shearing, and moisture. They often result from immobility or the use of a medical device. Pressure injuries remain a significant problem in acute and long-term care settings. Each year, more than 2.5 million patients in the United States are affected by hospital-acquired pressure injuries (HAPIs), formerly described as pressure ulcers or pressure sores, resulting in 60,000 deaths. Treating a single pressure injury can cost between $75,000 and $150,000, resulting in a combined $26.8 billion annually in the United States alone. A HAPI can result in significant patient harm, including costly treatments, increased pain, extended hospitalization, and increased morbidity and mortality. Up to 15% of patients admitted to the hospital will develop a pressure injury in the United States. Pressure injuries are especially prevalent in long-term (20–30%) and critical care settings (10–20%). CMS denies all reimbursements for HAPIs classified as stage III or IV. CMS has deemed these pressure injuries preventable and classifies them as never events. In addition to paying or reimbursing 0% for the treatment of these pressure injuries, CMS can also penalize hospitals with a 1% reduction in overall reimbursement for having an elevated HAPI rate if the hospital’s HAPI rate falls into the bottom 25% of hospitals nationwide (CMS, 2024; TJC, 2022; Mondragon & Zito, 2024; National Pressure Injury Advisory Panel [NPIAP], 2021).
Older adults have the highest rate of pressure injuries. Although older age alone is a contributing factor, the risk increases with comorbidities such as decreased mobility and activity level, impaired skin status, decreased oxygenation and perfusion, or increased skin moisture. Patients with mobility limitations, especially those confined to a bed or chair, have a higher risk of pressure injury development. Pressure injuries are of great concern to hospitalized patients, particularly those with limited mobility or on bed rest and those in long-term care facilities or home care. HCPs must complete a thorough head-to-toe skin assessment to determine HAPI risk properly. A comprehensive skin assessment includes skin temperature, color, moisture, turgor, and integrity. If any skin disruption is found, it should be identified, assessed, and documented thoroughly. A verified tool, such as the Braden or Norton Scale, should be used. These tools recognize the risk for pressure injuries and allow for ongoing, consistent assessment for risk or actual injury (AHRQ, 2014; NPIAP, 2019). Available risk tools examine contributing factors, including but not limited to:
- mobility and activity related to activities of daily living (ADLs)
- activity descriptors such as chairfast or bedfast
- factors affecting mobility, including weakness or paralysis
- increased friction or shear due to an inability to reposition (NPIAP, 2019)
Risk assessment should be repeated as indicated or based on patient location. The risk assessment should be performed every shift in acute care, weekly for 4 weeks, quarterly in long-term care facilities, and at every visit with a home care nurse. Staff should use the same tool consistently for all assessments. The plan of care should be developed with specific patient needs in mind. Patients and family members or caregivers should be educated on the care plan, as prevention and treatment will require a collaborative approach (AHRQ, 2014).
The prevention of pressure injuries is included in the TJC’s NPGs. TJC states that most pressure injuries can be avoided through preventive measures, and damage can be decreased if injuries are identified early. A multi-pronged approach to pressure injury prevention is the best practice. This includes addressing skincare, nutrition, repositioning and mobilization, and education (TJC, 2022, 2026c). Interventions that decrease the risk of pressure injuries are outlined in Table 6. For more information on this topic, please refer to the NursingCE activity entitled Pressure Injuries from Medical Devices and Hospitalization.
Table 6
Pressure Injury Prevention Points
Intervention | Explanation |
Skincare |
|
Nutrition |
|
Repositioning and mobilization |
|
Education |
|
(NPIAP, 2020)
Suicide
Worldwide, over 720,000 people die by suicide yearly, making it the third leading cause of death among individuals ages 15–29. Suicide is the 11th leading cause of death in the United States, the second leading cause of death among those aged 10–34, and the fourth leading cause of death among individuals between the ages of 35 and 44. More years of potential life are lost to suicide than to any other cause, except for heart disease, cancer, or unintentional injury. Suicide rates have increased by 30% from 2000 to 2020. In 2023, there were an estimated 1.5 million suicide attempts, resulting in 49,316 deaths. On average, 132 people die by suicide daily; a person dies every 11 minutes (a male every 14.1 minutes and a female every 51.3 minutes). There are 3.8 male deaths by suicide for every female death (American Foundation for Suicide Prevention [AFSP], 2023; CDC, 2025b; WHO, 2025).
While risk factors increase the likelihood of suicide, they are not always direct causes. Even among those who have risk factors for suicide, most people do not attempt suicide. While it remains difficult to predict who will act on suicidal thoughts, the risk for suicide rises as the number of contributing risk factors increases (AFSP, n.d.; CDC, 2024e). Other than a prior suicide attempt, the most well-cited risk factors for suicide include the following:
- General risk factors:
- social isolation or alienation
- recent or ongoing impulsive and aggressive tendencies or acts
- problems tied to sexual identity and relationships
- problems linked to other personal relationships
- Environmental influences:
- low socioeconomic status
- access to lethal means, including firearms and drugs
- barriers to accessing health care and treatment
- prolonged stress, such as harassment, bullying, relationship problems, or unemployment
- stressful life events like rejection, divorce, financial crisis, other life transitions, or loss
- exposure to another person’s suicide or graphic or sensationalized accounts of suicide
- Health factors:
- mental health conditions, such as:
- substance use disorder
- bipolar disorder
- schizophrenia
- hallucinations and delusions
- aggression, mood changes, and poor relationships
- conduct disorder
- depression
- anxiety disorders
- persons aged 18–25 years prescribed an antidepressant
- persons institutionalized for a mental health condition
- serious physical health conditions, including pain
- traumatic brain injury
- Historical risk factors:
- previous self-destructive behavior
- history of mood disorder(s)
- history of alcohol or other forms of substance misuse
- family history of suicide or psychiatric disorder(s)
- loss of a parent or loved one through any means
- history of trauma, abuse, violence, or neglect
- certain cultural or religious beliefs tied to suicide (AFSP, n.d.; CDC, 2024e; Suicide Awareness Voices of Education [SAVE], n.d.)
Suicide among patients receiving care in a facility staffed around the clock, including a hospital ED, or within 72 hours of discharge, is considered a sentinel event. TJC’s Sentinel Event database reports 126 suicides in 2024. An inadequate suicide risk assessment is the most commonly documented root cause. Other causes include insufficient staff-to-staff communication or transition of care and not following established policies regarding suicide prevention (TJC, 2024b). Since suicide is considered a sentinel event, when it occurs, the health care organization must perform an RCA to determine the cause(s), as shown in Figure 4.
Figure 4
RCA for Suicide
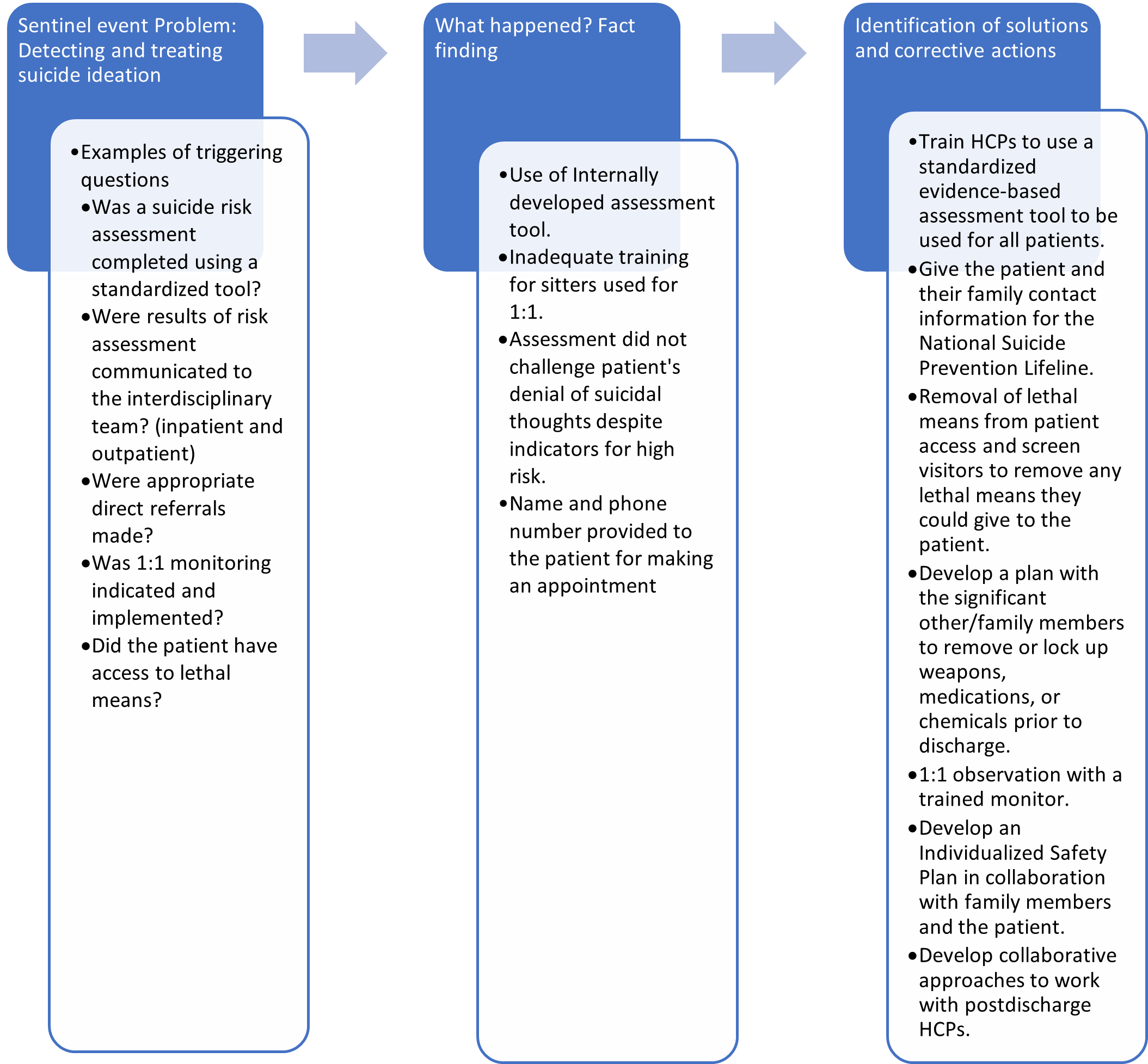
(adapted from TJC, 2025a)
Suicide Prevention
HCPs in primary, emergency, and behavioral health care specialties hold essential roles in detecting suicidal ideation in acute or nonacute care settings. Assessing suicide risk remains a challenge. The Zero Suicide Institute and the National Strategy for Suicide Prevention put forth the Zero Suicide (ZS) Model, which provides a framework to coordinate a multilevel approach to implementing evidence-based practices. ZS encourages HCPs to screen all patients for suicide risk on their first contact with an organization and at each subsequent encounter (Brodsky et al., 2018; National Action Alliance for Suicide Prevention, n.d.). The following list outlines the assessment of risk for suicide as compiled and adapted from the National Action Alliance for Suicide Prevention (2018) and the US Department of Health and Human Services (2021) guidelines:
- A suicide risk assessment should consider risk and protective factors that may increase or decrease the patient’s risk of suicide.
- Observing and reporting warning signs and evaluating suicidal thoughts, intent, behaviors, and other risk and protective factors should inform any decision about a referral to a higher level of care.
- A person’s mental state and suicidal ideation can fluctuate considerably over time. Therefore, people at risk for suicide should be reassessed regularly, especially if their circumstances have changed.
- The HCP should observe the patient’s behavior during the clinical interview. Disconnectedness may indicate an increased risk for suicide.
- The HCP should remain both empathetic and objective. A direct, nonjudgmental approach allows the HCP to gather the most reliable information collaboratively and encourages the patient to accept help.
The NPG Goal 8 identifies how to manage patients at risk for suicide. According to the report, for patients who screen positively for suicidal behaviors, TJC encourages HCPs to request permission to contact friends, family members, or other outpatient treatment providers. If the patient declines to consent, the Health Insurance Portability and Accountability Act (HIPAA) permits a clinician to make these contacts without the patient’s permission when they believe the patient may be a danger to themselves or others (TJC, n.d.-d; 2026c).
HCPs must be equipped to handle the stress of a suicide crisis in a calm, structured manner. As with any other emergency, HCPs should always remain with the patient. The goal of suicidal crisis management is to mitigate the patient’s acute risk of suicidal behaviors and maintain their safety. Individuals demonstrating warning signs and behaviors that raise suspicion of a suicide crisis should be immediately referred for admission to an inpatient facility, as specialty care is urgently needed (SAVE, n.d.). The following list highlights the priority actions HCPs should take to preserve the life of patients in an acute suicidal crisis (National Action Alliance for Suicide Prevention, 2018; National Institute of Mental Health, 2025; Suicide Prevention Resource Center, n.d.):
- One-on-one observation in a safe health care environment is essential for patients who are an acute suicidal threat.
- Personal and direct referrals to outpatient behavioral health and other providers for follow-up care should be expected within 1 week of the initial assessment. It should not be left up to the patients to make their appointments.
- All patients with suicidal ideations and their family members should be given the number to the National Suicide Prevention Lifeline (988, or text HOME to 741741), as well as local crisis and peer support contacts.
- Keep at-risk patients away from anchor points for hanging and materials that can be used for self-injury, such as bandages, sheets, restraint belts, plastic bags, elastic tubing, and oxygen tubing. This includes the screening of visitors.
- Conduct safety planning collaboratively with each patient to identify possible coping strategies. Resources for reducing risks should be identified and given to the patient. Evidence indicates that a “no-suicide contract” does not prevent suicide and is not recommended by experts in the field. The safety plan details should be reviewed with the patient at every interaction until the patient is no longer considered at risk for suicide.
- Restrict access to lethal means, such as firearms, knives, prescription medications, and chemicals. Discuss ways of removing or locking up firearms, possible weapons, medications, and chemicals with family members or significant others. Health care institutions should keep medications, chemicals, supplies, and equipment secured.
TJC also addresses behavioral health treatment following discharge. Evidence-based treatments and discharge plans must be implemented, and transition and follow-up care should be well coordinated with all providers (TJC, n.d.-d, 2026c).
- Establish a collaborative, ongoing, and systematic assessment and treatment process with the patient involving the patient’s other providers, family, and friends as appropriate.
- Develop specific treatment and discharge plans that directly target suicide prevention.
- Postdischarge prevention includes evidence-based interventions emphasizing patient engagement, collaborative assessment and treatment planning, problem-focused clinical intervention skills training, shared service responsibility, and proactive and personal clinician involvement in care transitions and follow-up care (TJC, n.d.-d, 2026c).
For more information on this topic, please refer to the NursingCE activity entitled Suicide and Suicide Prevention for Health Care Professionals.
Alarm Fatigue
Alarms are standard in many medical devices used in patient care, including electrocardiogram (ECG) machines, pulse oximetry devices, telemetry monitors, ventilators, and infusion pumps. Alarms are essential when providing safe patient care, but technology limitations often occur in practice. Alarm fatigue occurs when an HCP becomes desensitized to these alarms due to their prevalence in the clinical setting and the number of false and nonactionable alarms. Approximately 85–99% of alarm signals have no clinical significance or do not require clinical intervention. Per current estimates, nurses must respond to between 150 and 400 alarms per patient per shift, equating to approximately 35% of their time. In contrast, 40 years ago, the number of alarms per critical care patient per shift was 6. The desensitization and disruption can lead to decreased response times, resulting in poor patient outcomes (Lewandowska et al., 2023; Woo & Bacon, 2020). Contributing factors to alarm fatigue and poor patient outcomes include:
- different monitoring systems that have similar sounds
- default settings that are not adjusted to the patient population or the individual patient
- alarms become unreliable and disruptive, leading staff to decrease the volume, silence, or deactivate the alarms (Woo & Bacon, 2020)
Review Figure 5 for an RCA of Alarm Fatigue.
Figure 5
RCA-Alarm Fatigue
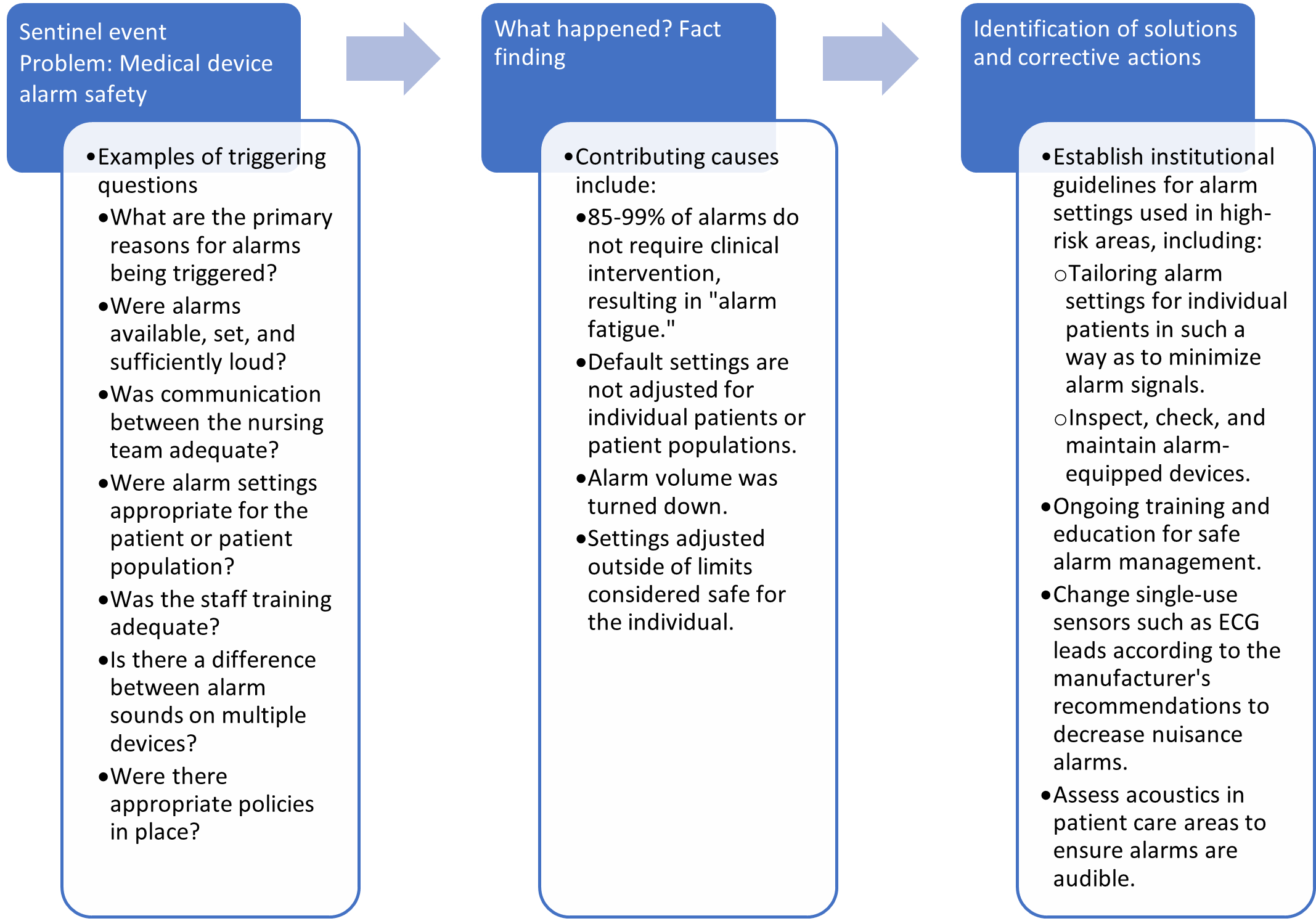
(adapted from TJC, 2013a)
Prevention of Alarm Fatigue Errors
Goal 1 of the 2026 NPGs (01.05.01) for hospitals addresses reducing patient harm due to clinical alarm systems. Preventing injury related to using medical devices equipped with alarms aims to reduce the chance of human error through training, technology, monitoring, and increased awareness. Institutions must demand that manufacturers of devices provide a variety of sounds so that alarms can be distinguished. An assessment of unit acoustics with correction of impediments to sounds being heard clearly must be conducted at the institutional level (TJC, 2013a, 2026c).
Multidisciplinary teams, including experts on human behavior, should be used to create policies and processes for setting and monitoring alarms at the initiation of device use and during hand-off communications. Settings for specific patient populations should be identified and communicated for patient-care units, and processes should be established for reviewing indications for individualized settings. For example, adjusting the preset delay of a pulse oximetry monitor from 5 to 10 seconds would decrease alarms caused by movement and temporary oxygen changes (AHRQ PSN, 2024a; TJC, 2013a). Ongoing training and education should be aimed at the following:
- changes in the technology used
- appropriate application and changing of sensors
- institutional policies and procedures
- processes for checking sensors and alarm settings
- tiered alerts for severity
- communication among the team members (AHRQ PSN, 2024a; TJC, 2013a, 2026c)
Surgical Errors
Examples of significant errors in a surgical setting include infection, WSPEs, and URFO. Approximately 4,000 surgical errors occur annually in the United States. Data analysis has identified that these events are often due to errors occurring before or after the procedure rather than mistakes made during the operation. WSPEs and URFO are two of the five most frequently reviewed sentinel events. URFOs are most commonly related to a lack of communication between staff members and a deviation from established facility policies and best practices. URFOs can lead to extended stays, surgical revisions, and patient harm. WSPEs can also be attributed to a lack of communication between team members and deviation from established policies, especially when performing a time-out before beginning every surgical procedure. WSPEs can result in severe, temporary, or permanent harm, including the death of the patient (TJC, 2026c; Rodziewicz et al., 2024; Santos & Jones, 2023). Surgical errors can lead to a sentinel event, causing the health care organization to implement an RCA to determine the cause(s). Figure 6 depicts an RCA identified by the TJC Sentinel Event Alert #51 involving the prevention of URFOs.
Figure 6
RCA-Unintended Retained Foreign Object
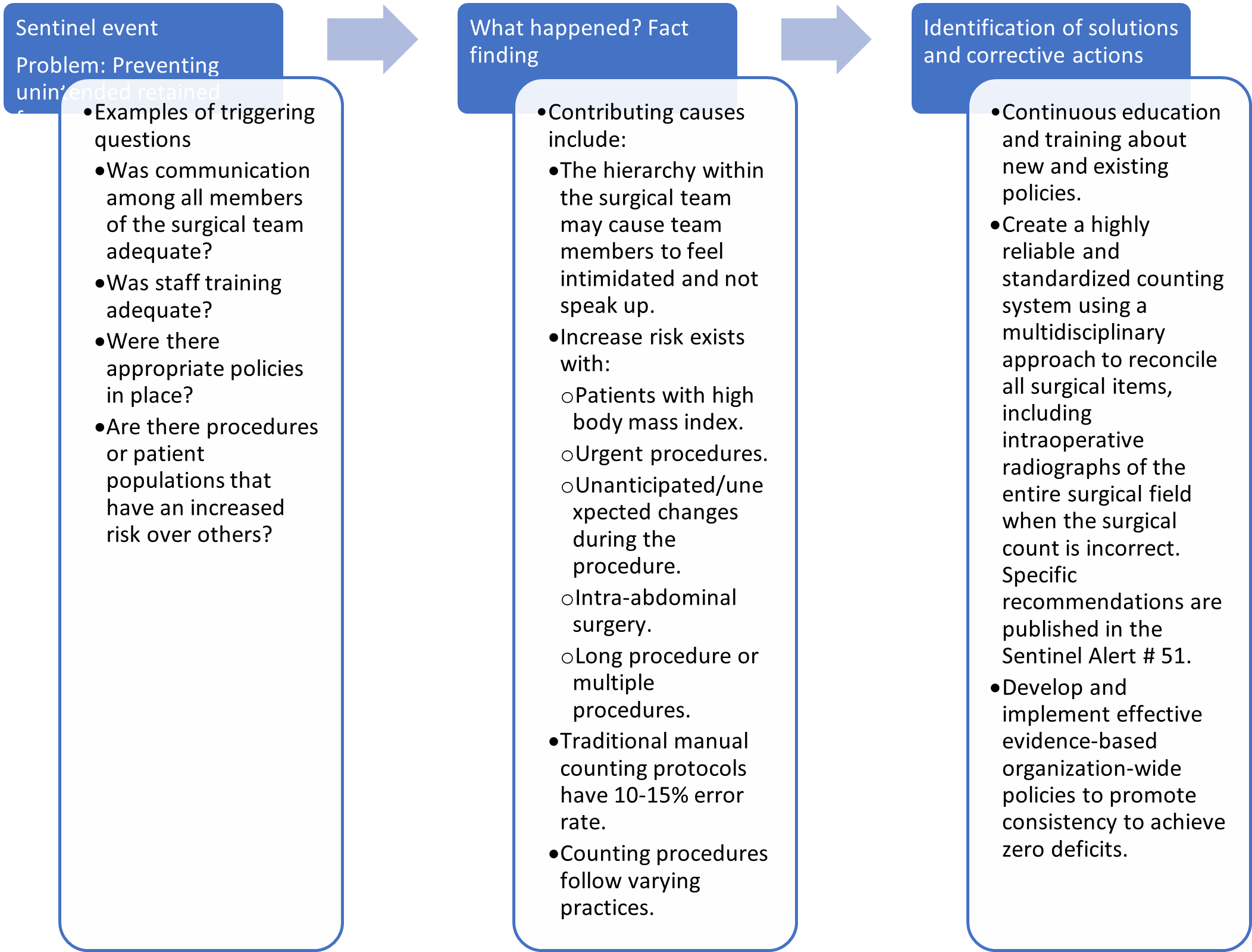
(adapted from TJC, 2013b)
Prevention of Surgical Errors
TJC 2026 NPGs outline measures to prevent surgical errors, including a universal protocol. This protocol supports using a time-out to review patient and surgical information to catch any possible WSPEs. When feasible, patients and their families should be included in this process to add another layer of protection against surgical errors. There also needs to be open and active communication between HCPs. The universal protocol to prevent surgical errors is most effective in health care environments that support teamwork and empower all individuals to advocate for patient safety, regardless of their title and role. Although a time-out procedure and active communication among HCPs can prevent WSPE errors, this technique will not prevent URFOs. To ensure that a URFO does not occur at the end of the procedure, the surgeon, anesthesiologist, and nurse must verbally count the number of instruments and sponges and ensure that the number matches the count created during the surgical procedure (TJC, 2026c; Rodziewicz et al., 2024; Santos & Jones, 2023).
Hand-Off Communication
Hand-off communication is inevitable, as one person cannot always be available; this is especially true in a hospital setting where nurses change shifts and providers may work as a team to care for the patient. Too often, individual HCP efforts to provide safe and effective care fail as the patient is handed off to another HCP for continuing care or services. Hand-off is the transfer and acceptance of patient care responsibility achieved through effective communication. It is a real-time process of passing patient-specific information from one caregiver to another to ensure the continuity and safety of the patient’s care. Effective hand-offs can be complex, and failures in this area have long been considered the root cause of various sentinel events, albeit not the sentinel event itself. Poor hand-off communication can lead to a lack of follow-up, missed or delayed treatment, and duplication of therapy or testing. The following root causes of poor hand-off communication were identified through the Robust Process Improvement project enacted in 10 hospitals: delays, inattention, lack of knowledge, lack of time, poor timing, interruptions, distractions, and lack of standardized procedures. Of malpractice claims, 49% were due to a communication failure, and these claims were less likely to be dropped or dismissed than malpractice claims citing a different medical error. Of these claims, approximately 47% resulted from ineffective provider communication (AHRQ PSN, 2024d; Humphrey et al., 2022; TJC, 2024a; Raeisi et al., 2019).
TJC has provided tips to assist caregivers in making high-quality handoffs. The following is a brief synopsis of the tips from Sentinel Alert issue #58 (TJC, 2017b).
- Determine the critical information that needs to be communicated.
- Use standardized tools to communicate.
- Do not rely only on electronic or paper communication. Face-to-face or phone communication allows the receiver to ask questions and seek clarification.
- Combine information from multiple sources and communicate at the same time.
- Verify that the receiver gets minimal essential information.
- Hand-off communication should occur in a designated “zone of silence” free from nonemergency interruptions.
- Include all team members in the hand-off and, if possible, the patient and their family members.
- Use electronic health records and other technologies to enhance communication, but do not rely solely on them.
Hand-off communication can lead to a sentinel event, causing the health care organization to implement an RCA to determine the cause(s). Figure 7 depicts an RCA identified by TJC Sentinel Event Alert #58 for inadequate hand-off communication.
Figure 7
RCA-Hand-Off Communication
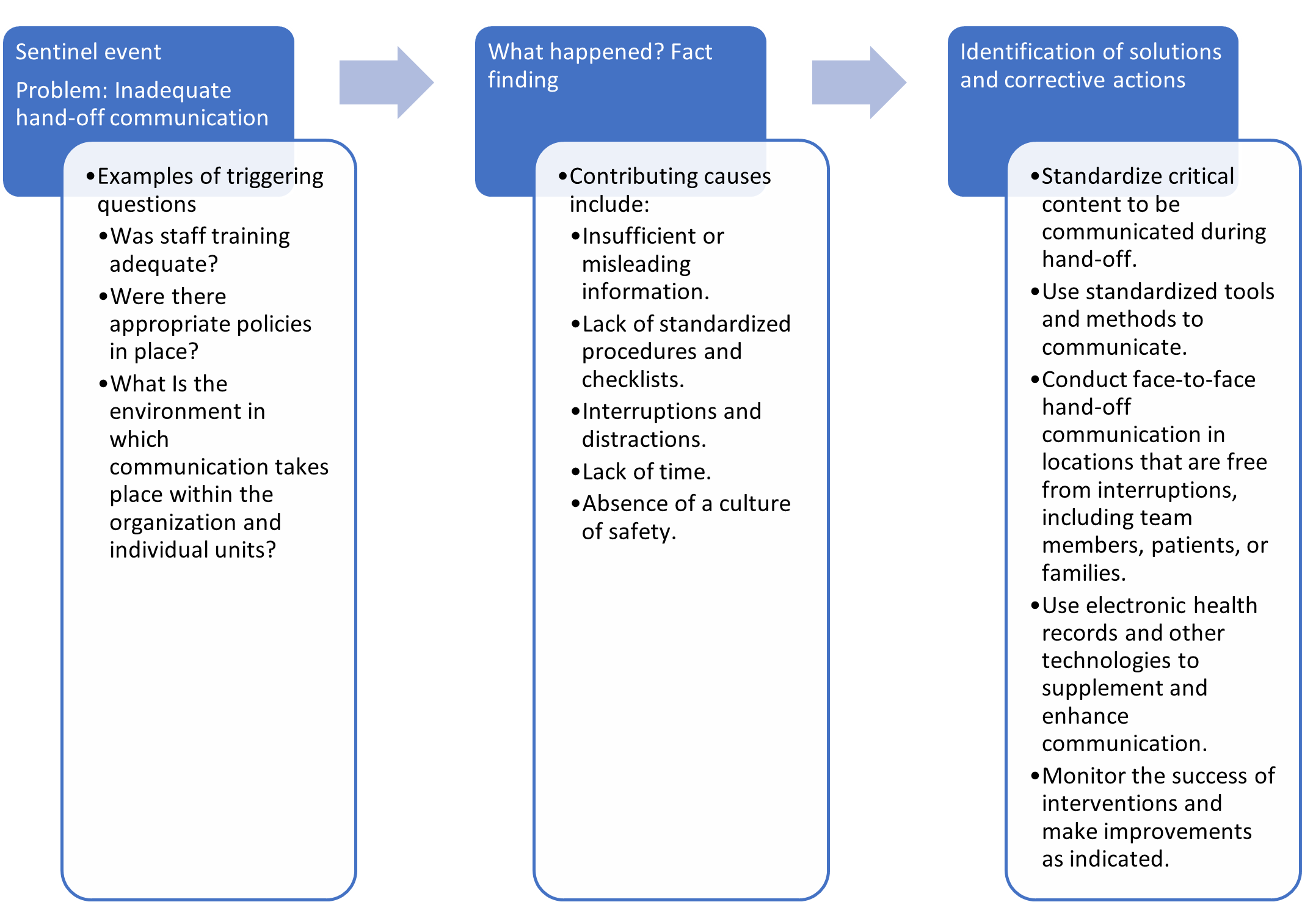
(adapted from TJC, 2017b)
Preventing Hand-Off Communication Errors
Effective communication needs to be supported throughout the entire organization. It requires sufficient time, staffing, and space; standardized tools and expectations; and the encouragement of questioning in a safe environment. Multidisciplinary teams should develop the protocols and tools for guiding communication between departments and disciplines. Protocols should favor face-to-face hand-offs; provide for quiet, uninterrupted environments; foster the participation of team members, including the patient; and promote the use of standardized tools to guide communication. Education and training should include role-playing sessions and follow-up monitoring for all members of the provider team. Institutions have been able to reduce ineffective hand-off communication and related adverse events significantly by using a variety of evidence-based communication checklists and tools, such as the SBAR tool and I-PASS (illness severity, patient summary, action list, situation awareness and contingency plans, synthesis by the receiver). The I-PASS tool is the gold standard of hand-off formats and has fostered effective communication between providers (AHRQ PSN, 2024d; TJC, 2017b).
Patient Identification
An error while identifying a patient can occur in any aspect of the health care system—such as clinical care, medication administration, or billing—and every health care setting, from hospitals to walk-in clinics and healthcare providers’ offices. HCPs are acutely aware of how egregious these errors are. Most patient identification mistakes are caught before the patient is harmed. However, research indicates that patient identification errors leading to temporary or permanent harm or death have occurred. TJC initially listed improving the accuracy of patient identification as one of their 2014 NPSGs, and it remains goal 1 of the 2026 NPGs (TJC, 2026c).
Problems commonly associated with patient identification errors can develop because the institution does not have formal policies outlining the procedure for proper patient identification, existing policies are not followed or enforced, or the policy’s intention is inadequate. When policies exist, the reasons most often given for noncompliance are time constraints, language barriers, and the use of yes/no questions (Choudhury & Vu, 2020). Patient identification errors most commonly occur in the following areas:
- registration (i.e., facilities that do not require photo identification during registration)
- wristband accuracy and use (i.e., missing, incorrect, incomplete, or poorly designed wristbands)
- order entry and charting (i.e., software issues or information placed in the wrong patient’s chart)
- medication administration (i.e., not following protocols before administering medications)
- surgery (i.e., WSPEs; Choudhury & Vu, 2020; Emergency Care Research Institute [ECRI], 2016; TJC, n.d.-f)
Research suggests that compliance with patient identification protocols when administering medications was higher among new nurses than among more experienced nurses. WSPEs occur due to communication or system errors often attributed to the diagnosis process when incorrect medical records, radiographs, or laboratory samples are used (ECRI, 2016; TJC, n.d.-f). Any of these patient misidentifications can lead to a sentinel event, causing the health care organization to implement an RCA to determine the cause(s). Figure 8 depicts an RCA identified by the NPG as Goal #1 for patient identification.
Figure 8
RCA-Incorrect Patient Identification
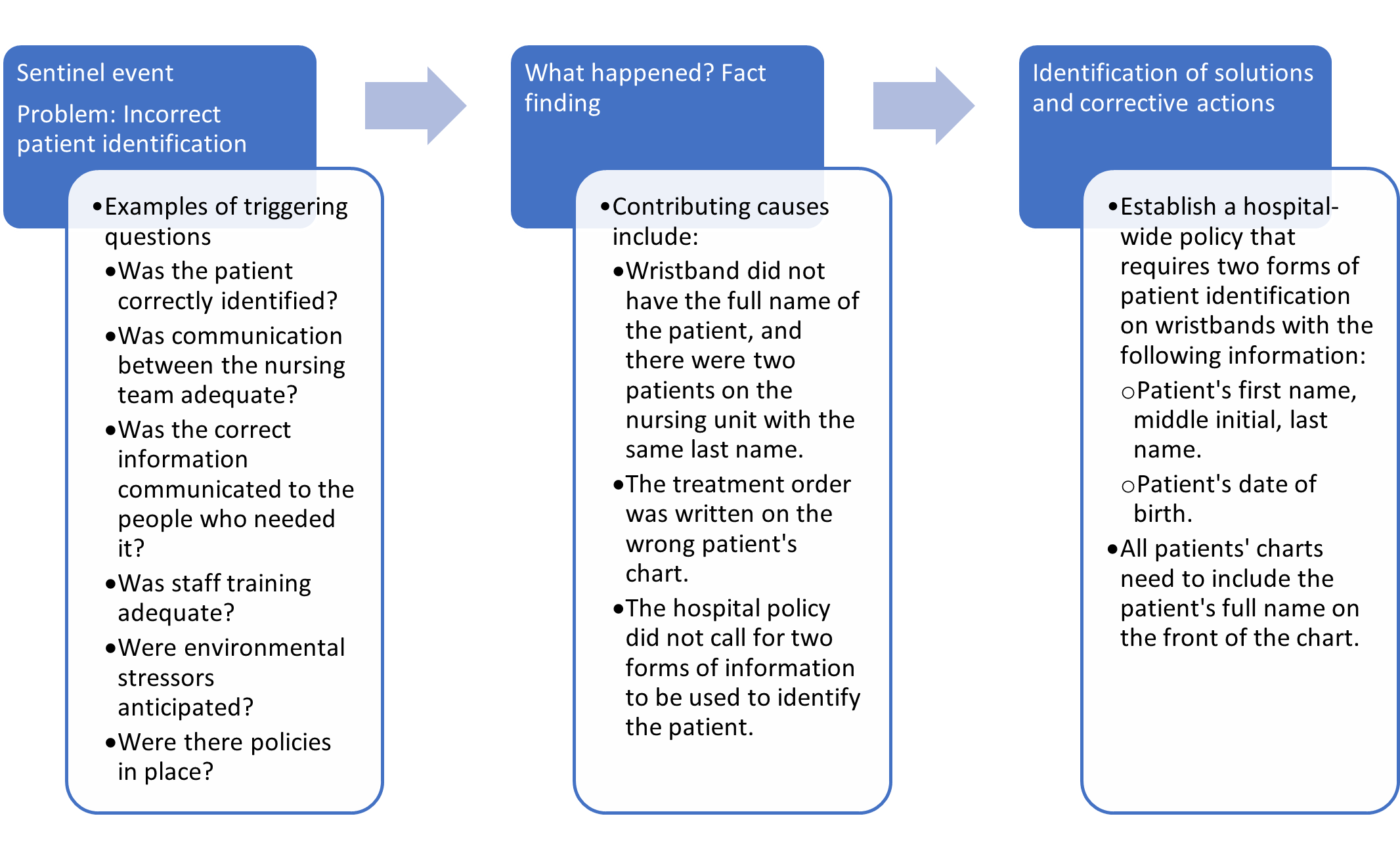
(adapted from TJC, n.d.-f, 2026c)
Prevention of Incorrect Patient Identifier Errors
The goal for improving patient identification accuracy is to identify the individual for whom the treatment is intended reliably, matching the treatment to the individual. This can be achieved by using two patient identifiers when administering medications and blood, collecting specimens for testing, and implementing treatments. Additionally, all containers used for blood and other specimens should be labeled in front of the patient. In addition, health care organizations should establish standardized approaches for patient identification, particularly within health care systems. Policies must be established and followed consistently, especially for identifying non-verbal patients and patients with the same name. When addressing a patient, nurses should avoid questions with yes/no answers. Patients may be embarrassed to admit they did not hear or understand the question, automatically answering “yes” as a result. Education is essential in preventing patient identification errors and must be incorporated into orientation and continuing education for all employees. Nurses can also involve patients and family members by educating the public regarding the risks of patient misidentification (ECRI, 2016; TJC, n.d.-f).
Leadership’s Role in Creating a Safety Culture
As noted in each of the NPG categories, much of the RCA process focuses on the systemic failures of the organization that led to the event in question. The leadership of each health care organization is accountable for creating and maintaining a safe environment for patients, employees, and visitors. Competent leaders recognize that systemic flaws or weaknesses exist in every organization; despite policies, protocols, and training, the potential for error exists because human factors are always a problem. Leadership failure contributes to many adverse events, such as ineffective hand-off communication, WSPEs, and delays in treatment. Goal 2 of the NPGs is focused on the governing body and leadership team fostering a culture of safety (TJC, 2026c).
Without an environment of safety with organizational support and monitoring, creating policies or purchasing the latest technology will not significantly reduce the number of adverse incidents or near misses. Improving an organization’s safety culture and removing punitive actions following the reporting of medical errors are essential to prevent and reduce the prevalence of medical errors. An environment of safety requires all health care team members to communicate, question, and confront concerns regardless of institutional hierarchy. All team members, regardless of title or tenure, must feel comfortable and supported to speak up when a circumstance arises that can lead to an error. Leaders should address unprofessional and bullying behavior to create a cultural shift to one of safety and to ensure that the required changes are sustained. This necessitates attention to attitudes, skills, and conditions over time (AHRQ, 2024b; Albright-Trainer et al., 2020; Mistri et al., 2023). A lack of an organizational culture of safety contributes to adverse outcomes by:
- inhibiting staff from reporting potential safety vulnerabilities
- giving little or no feedback and support to staff who report vulnerabilities
- allowing intimidation so that the report of adverse events is viewed as an incident that may result in punishment or retribution
- inconsistently prioritizing the implementation of safety regulations
- ignoring signs of staff burnout (AHRQ PSN, 2024b; Albright-Trainer et al., 2020; Mistri et al., 2023)
Leaders make organizational goals and values visible through everyday actions, including those related to patient safety. Inconsistencies between words and actions result in the inability to achieve the stated goals. Leaders must commit to behavior that accurately reflects an authentic culture of safety. No amount of resources or policies can create and maintain an environment or culture as effectively as leadership can. The organizational culture reflects daily actions and should be palpable to patients, staff, and anyone entering the organization (AHRQ PSN, 2024b; Albright-Trainer et al., 2020; Mistri et al., 2023).
Organizations with a quality safety culture have leaders who are deliberate in their actions to address safety issues. They consider safety issues as potential systemic problems, not a problem with the employees. They understand adverse events and near misses as providing “information-rich” data for analysis and systems improvement. Poor leadership is a contributing factor or root cause of reported sentinel events. To prevent future adverse events, leadership failures must be examined in the same way as a sentinel event (AHRQ PSN, 2024b; Albright-Trainer et al., 2020; Mistri et al., 2023). Leadership failure can lead to a sentinel event, causing the health care organization to implement an RCA to determine the cause(s). Figure 9 depicts an example of an RCA as identified by TJC Sentinel Event Alert #57 for leadership failure.
Figure 9
Leadership Failure in Sustaining a Safety Culture
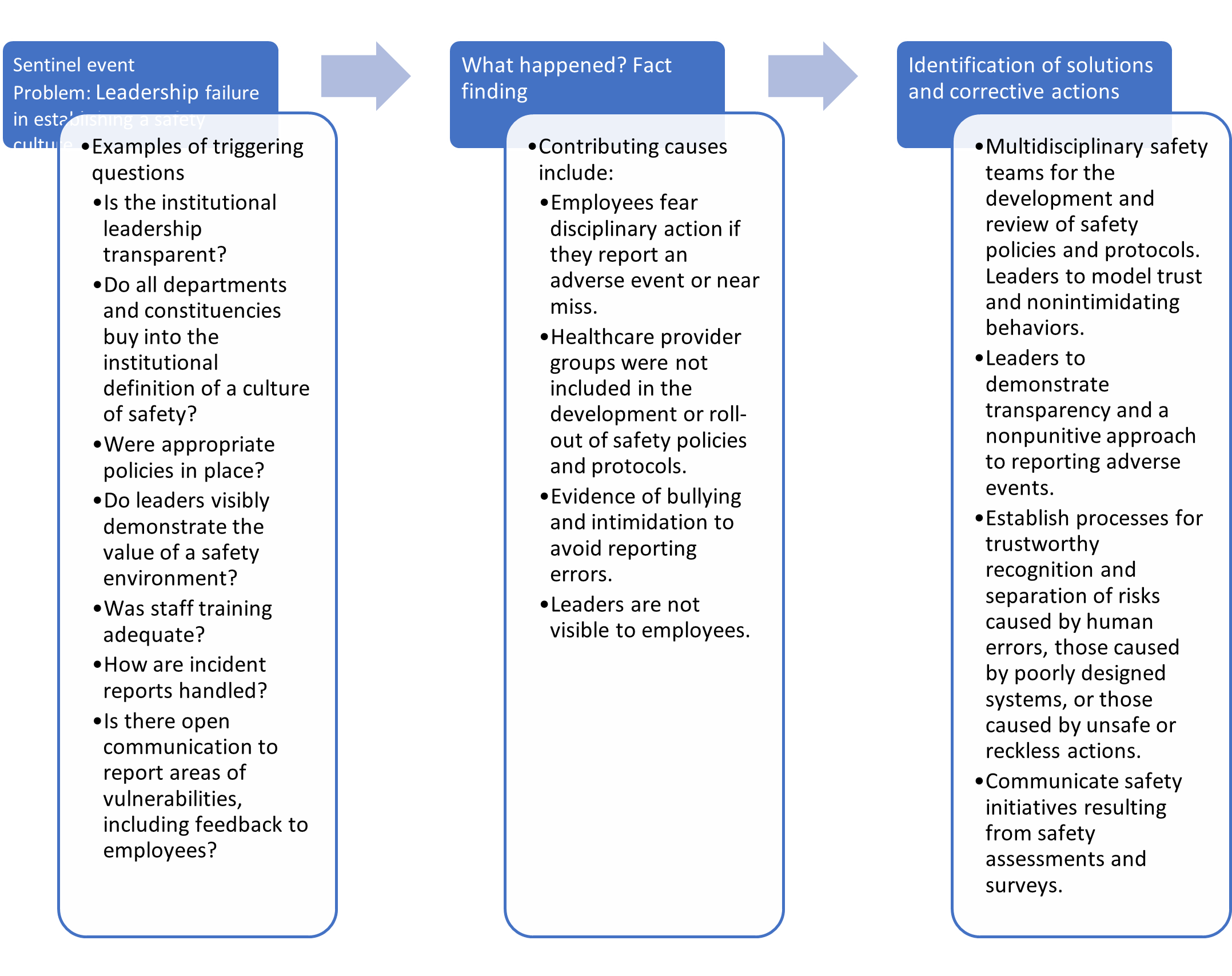
(adapted from TJC, 2017a)
Preventing Leadership Failure in Sustaining a Safety Culture
Within a successful organization, employees are encouraged—even rewarded—for providing essential safety-related information. Processes should differentiate between human error and at-risk or reckless behaviors. A culture that encourages employees to self-report their errors and near misses without punishment creates an atmosphere where consequences of errors can be minimized and systemic problems identified early. Treating everyone with dignity and respect is essential to developing a safe and effective environment. This leads to employees who are engaged, productive, and collaborative. An organization must focus on grooming and training its leadership team in the areas of institutional values for a culture of safety, leadership skills, and organizational communication. Transparency and accountability must be expected at all levels of the leadership team. All organization members’ feedback should be sought and integrated into the analysis of organizational safety systems. Leaders should listen to feedback and use it for improvement (TJC, 2017a; Sameera et al., 2021). TJC has made the following suggestions in their Sentinel Event Alert #57 for leadership that supports building a culture of safety:
- A transparent, nonpunitive approach to reporting and learning from adverse events, close calls, and unsafe conditions is crucial.
- Establish clear, just, and transparent risk-based processes for recognizing and separating human error and error arising from poorly designed systems from unsafe or reckless actions that are blameworthy.
- To advance trust within the organization, leaders must adopt and model appropriate behaviors and champion efforts to eradicate intimidating behaviors.
- Establish, enforce, and communicate to all team members the policies supporting the safety culture and the reporting of adverse events, close calls, and unsafe conditions.
- Positively recognize or reward care team members who report adverse events and close calls, identify unsafe conditions, or have good suggestions for safety improvements.
- Establish an organizational baseline measure of safety culture performance using the AHRQ Patient Safety Cultures Survey or the Safety Attitudes Questionnaire.
- Analyze safety culture survey results from across the organization to find quality and safety improvement opportunities.
- In response to information gained from safety assessments and/or surveys, develop and implement unit-based quality and safety improvement initiatives designed to improve the culture of safety.
- Embed safety culture team training into quality improvement projects and organizational processes to strengthen safety systems.
- Proactively assess system (i.e., medication management or electronic health records) strengths and vulnerabilities and prioritize them for enhancement or improvement.
- Repeat organizational assessment of safety culture every 18–24 months to review progress and sustain improvement (TJC, 2017a; Sameera et al., 2021).
Nurses’ Role and Responsibility Regarding the Prevention of Medical Errors
| Florida Nursing Alert: “Licensed Practical Nurses, Registered Nurses, Clinical Nurse Specialists, and Advanced Registered Nurse Practitioners are required to complete 24 hours of appropriate CE during each renewal period, including two (2) hours relating to the prevention of medical errors and two (2) hours in laws and rules in nursing. In addition to these 24 hours of general CE, every third renewal, two (2) hours of domestic violence CE must be completed for a total of 26 hours (Florida Board of Nursing, 2016)." |
In many states, including Florida, nurses must complete a continuing education course related to medical errors and their role. Nurses have a significant role in ensuring the safe delivery of patient care by identifying, interrupting, and correcting errors, thereby reducing and minimizing adverse or sentinel events. At the bedside, nurses are the primary defense against many errors that can adversely affect patients. Nurses can turn potentially adverse outcomes into near-miss events and prevent sentinel events. Nurses should be committed to creating a safe environment for their patients. There are many ways a medical error can occur. Some errors may involve systemic processes or other departments such as medical, pharmacy, or laboratory; nurses can be crucial in the identification and avoidance of potential errors (AHRQ PSN, 2024b; ANA, 2023; Henneman, 2017; Rodiewicz et al., 2024).
Nurses use several strategies to identify, interrupt, and correct medical errors. Nurses may identify errors through surveillance, double-checking, and knowledge of the patient, care plan, policies, and procedures. The surveillance strategy involves systematically and continuously observing each patient and their environment. Often, nurses will double-check provider orders or interventions with other nurses to ensure the order or intervention is appropriate and makes sense. Knowing the patient involves developing a relationship with the patient and family members, being knowledgeable about the patient’s medical history, maintaining continuity of care, and communicating with team members. Knowing the care plan involves developing and communicating the comprehensive care plan to others (e.g., during a change of shift report or patient rounds). Nurses can prevent medical errors by knowing the nursing unit and the institution’s policies and procedures (AHRQ PSN, 2024b; ANA, 2023; Henneman, 2017; Rodiewicz et al., 2024).
In addition to these strategies for reducing medical errors, nurses can prevent errors by being actively involved in various activities that reach all members of the health care team, as well as patients and their families. Education is critical in preventing medical errors, and nurses can be involved in teaching team members and patients about up-to-date best practices. Nurses can be instrumental in developing agency policies and procedures by serving on agency committees that set policies and procedures. Nurses can facilitate effective and clear communication about patient care needs in their leadership role within the care team. Technology, particularly informatics, has contributed to efficiency, effectiveness, and accuracy in reporting and preventing medical errors through barcoding, electronic health records, and the ability to communicate across various databases. Nurses who focus on each patient, identify breaks in care processes, seek solutions, employ best practices, and participate in lifelong learning significantly reduce medical errors and provide a safe environment for patients (AHRQ PSN, 2024b; ANA, 2023; Henneman, 2017; Rodiewicz et al., 2024).
Interrupting errors is another aspect of a nurse’s role. Each nurse’s experience and confidence level influence their ability to interrupt errors. Nurses often use three methods when interrupting errors: offering assistance, clarifying, and verbally interrupting. Offering assistance is a nonthreatening and supportive approach to make someone aware that they are about to make a mistake, versus direct confrontation. Clarifying should occur when nurses are unsure of a provider’s order or an aspect of the plan of care; asking for clarification often resolves the situation. Asking “why” is a tactful method of verbally interrupting an error. When the potential for a sentinel event is high, verbally interrupting the action is often the most direct method. When using this method, nurses should try not to embarrass the individual or cause the patient anxiety. Correcting a medical error should occur when identifying or interrupting the error was unsuccessful, and additional intervention is necessary. This third strategy deals with persevering, being physically present, reviewing the care plan, and referring to standards or experts. Nurses give their complete attention to the error and follow-up to ensure the patient remains at their highest level of functioning. When prior attempts to identify or interrupt the medical error fail, nurses can utilize the strategy of being physically present. Nurses may interact face-to-face with the providers or other team members involved. When nurses sense there has been an error (omission or commission) in the plan of care, it is their responsibility to raise questions. The last example of a strategy for nurses to correct errors is using resources such as referencing institution/nursing unit policies, accreditation/regulatory agency standards, or current literature. By citing information from an expert, nurses can help others understand a potential error constructively (Henneman, 2017).
References
Adler, S. (2026). Effects of poor communication in healthcare. The HIPAA Journal. https://www.hipaajournal.com/effects-of-poor-communication-in-healthcare
Agency for Healthcare Research and Quality. (2003). AHRQ’s patient safety initiative: Building foundations, reducing risk. https://archive.ahrq.gov/research/findings/final-reports/pscongrpt/psini2.html
Agency for Healthcare Research and Quality. (2014). Preventing pressure ulcers in hospitals. https://www.ahrq.gov/patient-safety/settings/hospital/resource/pressureulcer/tool/pu7b.html
Agency for Healthcare Research and Quality. (2019). AHRQ national scorecard on hospital-acquired conditions updated baseline rates and preliminary results 2014–2017. https://www.ahrq.gov/sites/default/files/wysiwyg/professionals/quality-patient-safety/pfp/hacreport-2019.pdf
Agency for Healthcare Research and Quality. (2025). Diagnostic excellence. https://qualityindicators.ahrq.gov/resources/diagnostic_excellence
Agency for Healthcare Research and Quality Patient Safety Network. (2021). Medication administration errors. https://psnet.ahrq.gov/primer/medication-administration-errors
Agency for Healthcare Research and Quality Patient Safety Network. (2024a). Alert fatigue. https://psnet.ahrq.gov/primer/alert-fatigue
Agency for Healthcare Research and Quality Patient Safety Network. (2024b). Culture of safety. https://psnet.ahrq.gov/primer/culture-safety
Agency for Healthcare Research and Quality Patient Safety Network. (2024c). Diagnostic errors. https://psnet.ahrq.gov/primers/primer/12
Agency for Healthcare Research and Quality Patient Safety Network. (2024d). Handoffs and signouts. https://psnet.ahrq.gov/primer/handoffs-and-signouts
Agency for Healthcare Research and Quality Patient Safety Network. (2024e). Medication errors and adverse drug events. https://psnet.ahrq.gov/primers/primer/23/medication-errors
Agency for Healthcare Research and Quality Patient Safety Network. (2024f). Medication reconciliation. https://psnet.ahrq.gov/primer/medication-reconciliation
Agency for Healthcare Research and Quality Patient Safety Network. (2024g). Systems approach. https://psnet.ahrq.gov/primer/systems-approach
Agency for Healthcare Research and Quality Patient Safety Network. (2024h). The ongoing journey to prevent patient falls. https://psnet.ahrq.gov/perspective/ongoing-journey-prevent-patient-falls
Agency for Healthcare Research and Quality Patient Safety Network. (2024i). Wrong-site, wrong-procedure, and wrong patient surgery. https://psnet.ahrq.gov/primers/primer/18/wrong-site-wrongprocedure-and-wrong-patient-surgery
Albright-Trainer, B., Dayal, R., Agarwala, A., & Pukenas, E. (2020). Effective leadership and patient safety culture. Anesthesia Patient Safety Foundation, 35(2). https://www.apsf.org/article/effective-leadership-and-patient-safety-culture
Alqenae, F. A., Steinke, D., & Keers, R. N. (2020). Prevalence and nature of medication errors and medication-related harm following discharge from hospital to community settings: A systematic review. Drug Safety, 43, 517–537. https://doi.org/10.1007/s40264-020-00918-3
Amaraneni, A., Chippa, V., Goldin, J., & Rettew, A. C. (2024). Anticoagulation safety. In StatPearls [Internet]. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK519025
Ambwani, S., Misra, A. K., & Kumar, R. (2019). Medication errors: Is it the hidden part of the submerged iceberg in our healthcare system? International Journal of Applied and Basic Medical Research, 9(3), 135–142. https://doi.org/10.4103/ijabmr.IJABMR_96_19
American Foundation for Suicide Prevention. (n.d.). Risk factors, protective factors, and warning signs. Retrieved January 12, 2026, from https://afsp.org/risk-factors-and-warning-signs
American Foundation for Suicide Prevention. (2023). Suicide statistics. https://afsp.org/suicide-statistics
American Nurses Association. (n.d.-a). ANA CAUTI prevention tool. Retrieved January 8, 2026, from https://www.nursingworld.org/practice-policy/work-environment/health-safety/infection-prevention/ana-cauti-prevention-tool
American Nurses Association. (n.d.-b). Streamlined evidence-based RN tool: Catheter associated urinary tract infection (CAUTI) prevention. Retrieved January 8, 2026, from https://www.nursingworld.org/globalassets/practiceandpolicy/innovation--evidence/clinical-practice-material/cauti-prevention-tool/anacautipreventiontool-final-19dec2014.pdf
American Nurses Association. (2023). Safety strategies every nurse leader needs to know. https://www.nursingworld.org/content-hub/resources/nursing-leadership/safety-in-nursing
Appeadu, M. K., & Bordoni, B. (2023). Falls and fall prevention in older adults. In StatPearls [Internet]. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK560761
Boddy, N., & Avery, A. J. (2023). A systems approach to the safety and efficiency of prescribing at the primary-secondary care interface. Future Healthcare Journal, 10(3), 205–210. https://doi.org/10.7861/fhj.2023-0074
Brodsky, B. S., Spruch-Feiner, A., & Stanley, B. (2018). The zero suicide model: Applying evidence-based suicide prevention practices to clinical care. Frontiers in Psychiatry, 9, 33. https://doi.org/10.3389/fpsyt.2018.00033
Burchum, J. R., & Rosenthal, L. D. (2024). Lehne’s pharmacology for nursing care (12th ed.). Elsevier.
Centers for Disease Control and Prevention. (2017). Intravascular catheter-related infection (BSI) prevention guidelines, 2011. https://www.cdc.gov/infection-control/hcp/intravascular-catheter-related-infection/
Centers for Disease Control and Prevention. (2024a). Clinical safety: Hand hygiene for healthcare workers. https://www.cdc.gov/clean-hands/hcp/clinical-safety/index.html
Centers for Disease Control and Prevention. (2024b). Facts about falls. https://www.cdc.gov/falls/data-research/facts-stats
Centers for Disease Control and Prevention. (2024c). Guideline for hand hygiene in healthcare settings (2002). https://www.cdc.gov/infection-control/hcp/hand-hygiene
Centers for Disease Control and Prevention. (2024d). HAI and antimicrobial use prevalence surveys. https://www.cdc.gov/healthcare-associated-infections/php/haic-eip/antibiotic-use.html
Centers for Disease Control and Prevention. (2024e). Risk and protective factors for suicide. https://www.cdc.gov/suicide/risk-factors/index.html
Centers for Disease Control and Prevention. (2025a). About HAIs. https://www.cdc.gov/healthcare-associated-infections/about/index.html
Centers for Disease Control and Prevention. (2025b). Suicide data and statistics. https://www.cdc.gov/suicide/facts/data.html
Centers for Medicare and Medicaid Services. (n.d.). Partnership for patients. Retrieved January 5, 2026, from https://www.cms.gov/priorities/innovation/innovation-models/partnership-for-patients
Centers for Medicare and Medicaid Services. (2020). CMS manual system. https://www.cms.gov/files/document/r200soma.pdf
Centers for Medicare and Medicaid Services. (2024). Hospital-acquired conditions. https://www.cms.gov/medicare/payment/fee-for-service-providers/hospital-aquired-conditions-hac
Choudhury, L. S., & Vu, C. T. (2020). Patient identification errors: A systems challenge. https://psnet.ahrq.gov/web-mm/patient-identification-errors-systems-challenge
Dawson, J. (n.d.). Do no harm: Diagnostic errors and the laboratory. The American Society for Clinical Laboratory Science. Retrieved December 28, 2025, from https://www.ascls.org/do-no-harm-diagnostic-errors-laboratory
DeVries, M. (2019). Insertion related infection prevention with vascular access devices. In N. Moureau (Ed.), Vessel health and preservation: The right approach for vascular access (pp. 133–145). Springer. https://doi.org/10.1007/978-3-030-03149-7_10
Emergency Care Research Institute. (2016). Patient identification errors. https://www.ecri.org/Resources/HIT/Patient%20ID/Patient_Identification_Evidence_Based_Literature_final.pdf
Florida Board of Nursing. (2016). Rule 64B9-5.011: Continuing education on prevention of medical errors. https://www.flrules.org/gateway/RuleNo.asp?title=CONTINUING%20EDUCATION%20REQUIREMENTS&ID=64B9-5.011
Gervasi, C., Perego, E., Galli, F., Torri, V., Castoldi, M., & Bombardieri, E. (2025). Prevention of falls in hospitalized patients—Evaluation of the effectiveness of a monitoring system (Verso Vision) developed with artificial intelligence. Frontiers in Digital Health, 7, 1548209. https://doi.org/10.3389/fdgth.2025.1548209
Gregory, B., & Kaprielian, V. S. (n.d.). QI patient safety—Quality improvement: Vocabulary. https://josieking.org/patientsafety/module_e/vocabulary.html
Griffin, T. (2023). Sentinel events. Society for Academic Specialists in General Obstetrics and Gynecology. https://sasgog.org/common-sources-of-improvement-work/sentinel-events
Haddadin, Y., Annamaraju, P., & Regunath, H. (2022). Central line-associated bloodstream infections. In StatPearls [Internet]. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK430891
Hanson, A., & Haddad, L. M. (2023). Nursing rights of medication administration. In StatPearls [Internet]. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK560654
Harris, E. (2024). Study: Polypharmacy nearly doubled in 20 years among older adults in US. JAMA, 332(7), 524. https://doi.org/10.1001/jama.2024.13387
Henneman, E. A. (2017). Recognizing the ordinary as extraordinary: Insight into the “way we work” to improve patient safety outcomes. American Journal of Critical Care, 26(4), 272–277. https://doi.org/10.4037/ajcc2017128
Henshaw, C. M., & Rassilyer-Bomers, R. (2023). Craven’s Fundamentals of nursing: Concepts and competencies for practice (10th ed.). Wolters Kluwer.
Howick, J., Bennett-Weston, A., Solomon, J., Nockels, K., Bostock, J., & Keshtkar, L. (2024). How does communication affect patient safety? Protocol for a systematic review and logic model. BMJ Open, 14(5), e085312. https://doi.org/10.1136/bmjopen-2024-085312
Humphrey, K. E., Sundberg, M., Milliren, C. E., Graham, D. A., & Landrigan, C. P. (2022). Frequency and nature of communication and handoff failures in medical malpractice claims. Journal of Patient Safety, 18(2), 130–137. https://doi.org/10.1097/PTS.0000000000000937
Ignatavicius, D. D., Workman, M. L., Rebar, C. R., & Heimgartner, N. M. (2023). Medical-surgical nursing: Concepts for clinical judgment and collaborative care (11th ed.). Elsevier.
Imam, T. H. (2024). Catheter-associated urinary tract infections (CAUTI). https://www.merckmanuals.com/professional/infectious-diseases/urinary-tract-infections-utis/catheter-associated-urinary-tract-infections
Institute for Healthcare Improvement. (2018). New thinking on medication reconciliation. https://www.ihi.org/library/blog/new-thinking-medication-reconciliation
Institute for Safe Medication Practices. (2024a). ISMP list of confused drug names. https://online.ecri.org/hubfs/ISMP/Resources/ISMP_ConfusedDrugNames.pdf
Institute for Safe Medication Practices. (2024b). ISMP list of high-alert medications in acute care settings. https://online.ecri.org/hubfs/ISMP/Resources/ISMP_HighAlert_AcuteCare_List.pdf
Institute of Medicine. (2000). To err is human: Building a safer health system. National Academy Press. https://www.ncbi.nlm.nih.gov/books/NBK225182
Jarding, E. K., & Makic, M. B. F. (2021). Central line care and management: Adopting evidence-based nursing interventions. Journal of PeriAnesthesia Nursing, 36(4), 328–333. https://doi.org/10.1016/j.jopan.2020.10.010
The Joint Commission. (n.d.-a). Framework for root cause analysis and corrective actions. Retrieved January 3, 2026, from https://digitalassets.jointcommission.org/api/public/content/3559a1e9d41842348122ca1f2c627e96?v=291853c9
The Joint Commission. (n.d.-b). Infection prevention and control & antibiotic stewardship. Retrieved January 12, 2026, from https://www.jointcommission.org/en-us/knowledge-library/infection-prevention-and-control-resource-center
The Joint Commission. (n.d.-c). Sentinel events. Retrieved December 28, 2025, from https://www.jointcommission.org/en-us/knowledge-library/sentinel-events
The Joint Commission. (n.d.-d). Suicide risk reduction. Retrieved January 13, 2026, from https://www.jointcommission.org/en-us/about-us/key-initiatives/suicide-risk-reduction
The Joint Commission. (n.d.-e). Targeted solutions tool (TST). Retrieved January 3, 2026, from https://www.jointcommission.org/en-us/products-and-services/high-reliability/targeted-solutions-tool
The Joint Commission. (n.d.-f). What are the key elements organizations need to understand regarding the use of two patient identifiers prior to providing care, treatment or services? Retrieved January 16, 2026, from https://www.jointcommission.org/en-us/knowledge-library/support-center/standards-interpretation/standards-faqs/000001545
The Joint Commission. (2003). Sentinel event alert 28: Infection control related sentinel events. https://www.jointcommission.org/en-us/knowledge-library/newsletters/sentinel-event-alert/issue-28
The Joint Commission. (2013a). Sentinel event alert 50: Medical device alarm safety in hospitals. https://www.jointcommission.org/en-us/knowledge-library/newsletters/sentinel-event-alert/issue-50
The Joint Commission. (2013b). Sentinel event alert 51: Preventing unintended retained foreign objects. https://www.jointcommission.org/en-us/knowledge-library/newsletters/sentinel-event-alert/issue-51
The Joint Commission. (2015). Sentinel event alert 55: Preventing falls and fall-related injuries in health care facilities. https://www.jointcommission.org/en-us/knowledge-library/newsletters/sentinel-event-alert/issue-55
The Joint Commission. (2017a). Sentinel event alert 57: The essential role of leadership in developing a safety culture. https://www.jointcommission.org/en-us/knowledge-library/newsletters/sentinel-event-alert/issue-57
The Joint Commission. (2017b). Sentinel event alert 58: Inadequate hand-off communication. https://www.jointcommission.org/en-us/knowledge-library/newsletters/sentinel-event-alert/issue-58
The Joint Commission. (2019). Sentinel event alert 61: Managing the risks of direct oral anticoagulants. https://www.jointcommission.org/en-us/knowledge-library/newsletters/sentinel-event-alert/issue-61
The Joint Commission. (2020). Root cause analysis in health care: A Joint Commission guide to analysis and corrective action of sentinel and adverse events (7th ed.). https://store.jcrinc.com/root-cause-analysis-in-health-care-a-joint-commission-guide-to-analysis-and-corrective-action-of-sentinel-and-adverse-events-7th-edition
The Joint Commission. (2022). Preventing pressure injuries. https://digitalassets.jointcommission.org/api/public/content/Quick-Safety-25-UPDATE-3-21-22?v=4bcdf311
The Joint Commission. (2024a). Reducing handoff communication failures and inequities in healthcare. https://www.globenewswire.com/news-release/2024/08/22/2934465/0/en/Reducing-Handoff-Communication-Failures-and-Inequities-in-Healthcare.html
The Joint Commission. (2024b). Sentinel event data 2024 annual review. https://digitalassets.jointcommission.org/api/public/content/eac7511986c0442a9c1ae04b1aa02cc0?v=ad34daa0
The Joint Commission. (2025a). R3 report: Requirement, rationale, reference. https://digitalassets.jointcommission.org/api/public/content/459bbe2be1ab4e5082b8a8d49d0c94e0
The Joint Commission. (2025b). Sentinel event policy (SE). https://digitalassets.jointcommission.org/api/public/content/4035922bcc2f41bd83fbc1f55764a7b4?v=bf31f43b
The Joint Commission. (2026a). National patient safety goals. https://www.jointcommission.org/en-us/standards/national-patient-safety-goals
The Joint Commission. (2026b). National performance goals (NPGs). https://www.jointcommission.org/en-us/standards/national-performance-goals
The Joint Commission. (2026c). National performance goals: Effective January 2026 for the hospital program. https://digitalassets.jointcommission.org/api/public/content/9ca80055182b4274842a5780a94f2c82?v=149a13a9&_gl=1*1bxdwah*_gcl_au*MTU1MjE0MjY2Mi4xNzY4MzIxMzgz*_ga*MTQ0NzkwMTU1My4xNzY4MzIxMzgz*_ga_K31T0BHP4T*czE3NjgzOTk4MzUkbzQkZzEkdDE3Njg0MDA3NTgkajEyJGwwJGgw
The Joint Commission Center for Transforming Healthcare. (n.d.). Targeted Solutions Tool® (TST®) hand-off communication. Retrieved January 8, 2026, from https://www.preventsuicidewi.org/Data/Sites/17/media/zero-suicide/zs-2018-2019/hand-off-communication-tst-fact-sheet-8-15.pdf
Lancaster, R. J., Vizgirda, V., Quinlan, S., & Kingston, M. B. (2022). To err is human, just culture, practice, and liability in the face of nursing error. Nurse Leader, 20(5), 517–521. https://doi.org/10.1016/j.mnl.2022.06.010
LeLaurin, J. H., & Shorr, R. I. (2019). Preventing falls in hospitalized patients. Clinics in Geriatric Medicine, 35(2), 273–283. https://doi.org/10.1016/j.cger.2019.01.007
Lewandowska, K., Medrzycka-Dabrowska, W., Tomaszek, L., & Wujtewicz,, M. (2023). Determining factors of alarm fatigue among nurses in intensive care units—A Polish pilot study. Journal of Clinical Medicine, 12(9), 3120. https://doi.org/10.3390/jcm12093120
Lodato, P., Goldstein, N. D., Mapp, A. M., Gbadebo, A., & Pearlman, S. A. (2025). Risk factors for unexpected death in patients identified by a communication and resolution program. Frontiers in Health Services, 5, 1712574. https://doi.org/10.3389/frhs.2025.1712574
Lynch, S. S. (2025a). Adverse drug reactions. https://www.merckmanuals.com/professional/clinical-pharmacology/concepts-in-pharmacotherapy/adverse-drug-reactions
Lynch, S. S. (2025b). Medication errors. https://www.merckmanuals.com/professional/clinical-pharmacology/concepts-in-pharmacotherapy/medication-errors
Mistri, I. U., Badge, A., & Shahu, S. (2023). Enhancing patient safety culture in hospitals. Cureus, 15(12), e51159. https://doi.org/10.7759/cureus.51159
Mondragon, N., & Zito, P. M. (2024). Pressure injury. In StatPearls [Internet]. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK557868
Monegro, A. F., Muppidi, V., & Regunath, H. (2023). Hospital-acquired infections. In StatPearls [Internet]. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK441857
Murphy, S. L., Kochanek, K. D., Xu, J., & Arias, E. (2024). NCHS data brief 521: Mortality in the United States, 2023. National Center for Health Statistics. https://www.cdc.gov/nchs/products/databriefs/db521.htm
Murray, J. S., Clifford, J., Larson, S., Lee, J. K., & Sculli, G. L. (2022). Implementing just culture to improve patient safety. Military Medicine, 188(7–8), 1596–1599. https://doi.org/10.1093/milmed/usac115
Naseralallah, L., Koraysh, S., Alasmar, M., & Aboujabal, B. (2025). The role of the pharmacists in mitigating medication errors in the perioperative setting: A systematic review. Systematic Reviews, 14(1), 12. https://doi.org/10.1186/s13643-024-02710-1
National Action Alliance for Suicide Prevention. (n.d.). Zero suicide. Retrieved January 13, 2026, from https://theactionalliance.org/healthcare/zero-suicide
National Action Alliance for Suicide Prevention. (2018). Recommended standard care for people with suicide risk: Making health care suicide safe. https://theactionalliance.org/sites/default/files/action_alliance_recommended_standard_care_final.pdf
National Alliance for Caregiving. (n.d.). Falls prevention conversation guide for caregivers. National Council on Aging. Retrieved January 10, 2026, from https://www.caregiving.org/wp-content/uploads/2020/05/FallsPrevention_FINAL.pdf
National Coordinating Council for Medication Error Reporting and Prevention. (n.d.). About medication errors. Retrieved December 28, 2025, from https://www.nccmerp.org/about-medication-errors
National Council of State Boards of Nursing. (2023). Next generation NCLEX-RN test plan. https://www.ncsbn.org/public-files/2023_RN_Test%20Plan_English_FINAL.pdf
National Healthcare Safety Network. (2026a). National healthcare safety network (NHSN) patient safety component manual. Centers for Disease Control and Prevention. https://www.cdc.gov/nhsn/pdfs/pscmanual/pscmanual_current.pdf
National Healthcare Safety Network. (2026b). Surgical site infection event (SSI). Centers for Disease Control and Prevention. https://www.cdc.gov/nhsn/pdfs/pscmanual/9pscssicurrent.pdf
National Institute of Mental Health. (2025). Suicide. https://www.nimh.nih.gov/health/statistics/suicide
National Patient Safety Foundation. (2015). RCA2: Improving root cause analyses and actions to prevent harm. https://www.ashp.org/-/media/assets/policy-guidelines/docs/endorsed-documents/endorsed-documents-improving-root-cause-analyses-actions-prevent-harm.ashx
National Pressure Injury Advisory Panel. (2019). Prevention and treatment of pressure ulcers/injuries: Clinical practice guideline. https://www.biosanas.com.br/uploads/outros/artigos_cientificos/127/956e02196892d7140b9bb3cdf116d13b.pdf
National Pressure Injury Advisory Panel. (2020). Pressure injury prevention points. https://cdn.ymaws.com/npiap.com/resource/resmgr/online_store/1a._pressure-injury-preventi.pdf
National Pressure Injury Advisory Panel. (2021). 2021 fact sheet: About pressure injuries in US healthcare. https://cdn.ymaws.com/npiap.com/resource/resmgr/public_policy_files/npiap_word_fact_sheet_08mar2.pdf
Nickel, B., Gorski, L., Kleidon, T., Kyes, A., DeVries, M., Keogh, S., Meyer, B., Sarver, M. J., Crickman, R., Ong, J., Clare, S., & Hagle, M. E. (2024). Infusion therapy standards of practice, 9th edition. Journal of Infusion Nursing, 47(1S), S1–S285. https://doi.org/10.1097/NAN.0000000000000532
Office of Disease Prevention and Health Promotion. (n.d.). Healthcare-associated infections workgroup. US Department of Health and Human Services. Retrieved January 8, 2026, from https://odphp.health.gov/healthypeople/about/workgroups/healthcare-associated-infections-workgroup
Ottosen, K., & Bucknall, T. (2024). Understanding an epidemiological view of a retrospective audit of medication errors in an intensive care unit. Australian Critical Care, 37(3), 429–435. https://doi.org/10.1016/j.aucc.2023.04.004
Patel, R. H., & Goldin, J. (2025). Medical error prevention and root cause analysis. In StatPearls [Internet]. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK570638
Patra, K. P., & De Jesus, O. (2023). Sentinel event. In StatPearls [Internet]. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK564388
Raeisi, A., Rarani, M. A., & Soltani, F. (2019). Challenges of patient handover process in healthcare services: A systematic review. Journal of Education and Health Promotion, 8, 173. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6796291
Rahmani, K., Garikipati, A., Barnes, G., Hoffman, J., Calvert, J., Mao, Q., & Das, R. (2022). Early prediction of central line associated bloodstream infection using machine learning. American Journal of Infection Control, 50(4), 440–445. https://doi.org/10.1016/j.ajic.2021.08.017
Rasool, M. F., Rehman, A., Imran, I., Abbas, S., Shah, S., Abbas, G., Khan, I., Shakeel, S., Hassali, M. A. A., & Hayat, K. (2020). Risk factors associated with medication errors among patients suffering from chronic disorders. Frontiers in Public Health, 8, 531038. https://doi.org/10.3389/fpubh.2020.531038
Robichaux, C., & Vittone, S. (2023). Ethics: Addressing error: Partnership in a just culture. The Online Journal of Issues in Nursing, 28(2). https://doi.org/10.3912/OJIN.Vol28No02EthCol01
Rodziewicz, T. L., Houseman, B., Vaqar, S., & Hipskind, J. E. (2024). Medical error reduction and prevention. In StatPearls [Internet]. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK499956
Sameera, V., Bindra, A., & Rath, G. P. (2021). Human errors and their prevention in healthcare. Journal of Anaesthesiology Clinical Pharmacology, 37(3), 328–335. https://doi.org/10.4103/joacp.JOACP_364_19
Santos, G., & Jones, M. W. (2023). Prevention of surgical errors. In StatPearls [Internet]. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK592394
Suicide Awareness Voices of Education. (n.d.). Warning signs of suicide. Retrieved January 13, 2026, from https://save.org/about-suicide/warning-signs-risk-factors-protective-factors
Suicide Prevention Resource Center. (n.d.). Respond effectively to individuals in crisis. Retrieved January 13, 2026, from https://sprc.org/effective-prevention/a-comprehensive-approach-to-suicide-prevention/respond-effectively-to-individuals-in-crisis/
Tariq, R. A., Vashisht, R., Sinha, A., & Scherbak, Y. (2024). Medication dispensing errors and prevention. In StatPearls [Internet]. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK519065
US Department of Health and Human Services. (2021). The surgeon general’s call to action to implement the national strategy for suicide prevention. https://www.hhs.gov/sites/default/files/sprc-call-to-action.pdf
Wiegmann, D. A., Wood, L. J., Cohen, T. N., & Shappell, S. A. (2022). Understanding the “Swiss Cheese Model” and its application to patient safety. Journal of Patient Safety, 18(2), 119–123. https://doi.org/10.1097/PTS.0000000000000810
Wisconsin Technical College System. (2023). 15.2 Basic concepts of administering medications. Retrieved January 8, 2026, from https://wtcs.pressbooks.pub/nursingskills/chapter/15-2-basic-concepts-of-administering-medications
Woo, M., & Bacon, O. (2020). Alarm fatigue. Agency for Healthcare Research and Quality. https://www.ahrq.gov/sites/default/files/wysiwyg/research/findings/making-healthcare-safer/mhs3/alarm-fatigue-1.pdf
World Health Organization. (n.d.). Medication without harm. Retrieved January 5, 2025, from https://www.who.int/initiatives/medication-without-harm
World Health Organization. (2025). Suicide. https://www.who.int/news-room/fact-sheets/detail/suicide
Yılmaz, A., & Sönmez, B. (2024). Nurses’ perspectives and experiences on medical errors: A qualitative study. Journal of Evaluation in Clinical Practice, 30(6), 1153–1164. https://doi.org/10.1111/jep.14125
Zhu, J., & Weingart, S. N. (2025). Prevention of adverse drug events in hospitals. UpToDate. Retrieved December 28, 2025, from https://www.uptodate.com/contents/prevention-of-adverse-drug-events-in-hospitals
Powered by Froala Editor