About this course:
This module explores the nurse’s role in safe and effective patient care through prioritization and delegation.
Course preview
Prioritization in Nursing
This module explores the nurse’s role in safe and effective patient care through prioritization and delegation.
Upon completion of this module, learners should be able to:
- discuss the importance of prioritization in delivering patient care
- explore the application of various prioritization frameworks and principles of delegation for safe, effective patient care
- apply the concepts of various prioritization frameworks and principles of delegation to case scenarios
Nurses are responsible for offering high-quality, evidence-based care to optimize patient outcomes. As new treatments emerge, people are living longer, healthier lives. As the US population ages, more people live with chronic health conditions. These conditions have created a clinical environment that is more complex than ever before. The demands of the complex clinical environment require that nurses multitask, prioritize, delegate, and make sound clinical decisions when providing patient care. The Centers for Disease Control and Prevention (CDC, 2025) defines chronic diseases as conditions that last more than 1 year, require ongoing medical attention, and/or limit activities of daily living (ADLs). Chronic disease is the leading cause of illness, death, and disability in the United States. An estimated 75% of American adults have at least one chronic disease, and 50% have two or more chronic diseases. Chronic conditions such as heart disease, cancer, chronic lung disease, diabetes mellitus, Alzheimer’s disease, and chronic kidney disease contribute significantly to the increasing complexity of care in the clinical environment. These chronic conditions contribute to $4.9 trillion in annual health care costs (CDC, 2024, 2025; Manetti, 2019).
New graduate nurses entering the clinical setting encounter various challenges in delivering safe and effective patient care. It is estimated that only 8% of new graduate nurses are prepared to make entry-level clinical judgments, creating an education-to-practice gap. In a 2020 survey, 66% of practicing nurses believed that nurse graduates are less prepared to enter practice than those graduating 5–10 years ago. Poor clinical judgment can lead to poor patient outcomes. New graduate nurses must receive focused training and clinical insight into promptly and appropriately identifying and prioritizing patient needs. This skill set requires knowledge about medical conditions and disease processes, the principles of medication administration, pharmacokinetics, and adverse effects, as well as the ability to appropriately apply this information to meet individual patient needs. Experienced nurses have acquired and developed clinical judgment through their experience delivering patient care. Due to staffing and resource shortages, new graduate nurses are expected to hit the ground running, delivering safe and effective care in a fast-paced health care environment with high patient acuity, high patient-to-nurse ratios, and complex clinical conditions despite their lack of experience. To ensure that new graduate nurses are prepared for these demands on entering the clinical setting, nurses must assess the clinical environment and apply appropriate prioritization frameworks and principles of delegation. In addition, recurrent application and intentional practice of clinical judgment must occur during their education (Kavanagh & Szweda, 2017; McGarity et al., 2023; Rebelo, 2020; Rose, 2022).
Prioritization in Nursing Care
Nursing programs devote significant time and attention to teaching nursing students how to prioritize their time to deliver safe and effective care. While in school, most clinical training involves caring for one or two patients with oversight from faculty and nurse preceptors. However, once the graduate nurse is in the clinical setting, they are often faced with a much higher patient load, and many things demand their attention. Prioritizing and managing time is vital for any successful novice or expert nurse. However, prioritizing and managing time are not necessarily skills that can be memorized or easily taught in a textbook. Nurses must combine knowledge and skills to make safe decisions when delivering care to a group of patients. However, the increasing complexity of patient situations and high patient-to-nurse ratios have hindered new graduate nurses from successfully prioritizing care, leading to avoidable errors and poor patient outcomes. This education-to-practice gap has been attributed to a lack of clinical reasoning and judgment in new graduate nurses. As a result, the National Council of State Boards of Nursing (NCSBN) launched the NexGen NCLEX in 2023 as an intentional initiative to focus the prelicensure assessment and determination of competency for clinical reasoning and judgment skills (Fernaays, 2024; Jessee, 2019; Kavanagh & Szweda, 2017; NCSBN, 2023).
The quality of patient care depends on nurses who are prepared to recognize patient needs and respond accordingly. Nursing judgment directly impacts the ability to apply evidence-based practice (EBP) and to react to changes in the patient’s condition. Hospitals have acknowledged the lack of new nurse preparedness for years and implemented extended orientations, preceptorships, mentoring programs, and nurse residency programs to bridge the gap between the education and practice settings. Despite organizational strategies to improve the safety and efficacy of patient care, preventable health care errors are the third leading cause of death in the United States. The transition from novice nurse to an advanced beginner is filled with insecurities and a lack of experienced and clinical judgment. Both patients and medical facilities benefit from nurses who can demonstrate competent clinical judgment (Mohamed & Al-Hmaimat, 2024; Nursing Education Staff, 2024). Researchers have found that only 13% of preceptors believed novice nurses could establish priorities and demonstrate safe nursing care. High-quality patient care depends on the nurse’s competence and application of clinical judgment (Fernaays, 2024). The NCSBN targets optimal outcomes for patients, nurses, and clinical organizations. Nurses should enter practice with the ability to make appropriate clinical decisions through clinical judgment (NCSBN, 2019).
It is not unusual for a nurse working on a general medicine or surgical unit to be tasked with caring for up to five or six patients with serious illnesses in a given shift. When managing these multipatient, complex care situations, nurses must be able to prioritize patient needs accurately to promote positive patient outcomes. Once the nurse receives their patient assignment, they must determine how to proceed with the shift and meet the multifaceted demands, including patient assessments, administration of medications, patient advocacy, the delegation of appropriate tasks to other...
...purchase below to continue the course
- Clinical Judgment
- While several terms are used interchangeably to describe the competencies needed to deliver safe and effective patient care, they have different meanings; nursing leadership should understand the distinctions among them to foster clinical judgment for new graduate nurses (Alfaro-Lefevre, 2019). The following terms are interrelated and represent essential processes that lead to the comprehensive application of EBP (Alfaro-Lefevre, 2019; Connor et al., 2022).
- Critical thinking is a broad term that includes reasoning inside and outside the clinical setting.
- Clinical reasoning is the process used to consider issues at the patient’s bedside or point of care to prevent or manage a problem.
- Clinical judgment is a nurse’s conclusion, decision, or opinion after considering all available data based on reflection, critical thinking, and clinical reasoning.
There have been conversations on the use of critical thinking versus the nursing process by nurse education experts. The American Nurses Association (ANA) standards state that the nursing process serves as a critical thinking model that promotes the competent care of patients (ANA, 2021). Critical thinking, which leads to clinical reasoning and ultimately clinical judgment, is purposeful and informed outcome thinking that:
- is guided by standards, policies, ethical codes, and laws
- is driven by patient, family, and community needs, as well as nurses’ needs to give competent and efficient care
- is based on principles of the nursing process, problem-solving, and the scientific method
- focuses on safety and quality, constantly re-evaluating, self-correcting, and striving to improve
- carefully identifies the key problems, issues, and risks involved while including patients, families, and key stakeholders in decision-making early in the process
- uses logic, intuition, and creativity and is grounded in specific knowledge, skills, and experience
- calls for strategies that make the most of human potential and compensate for problems created by human nature (e.g., finding ways to prevent errors, using technology, and overcoming the powerful influence of personal views; Alfaro-Lefevre, 2019; ANA, 2024)
In 1985, Patricia Benner first noted that critical thinking was based on attitudes and skills relative to logic, rationality, and reasoning (Benner et al., 2009). A person’s knowledge, skills, and attitudes (KSAs) drive critical thinking. The Quality and Safety Education for Nurses (QSEN, n.d.) competencies, which focus on positive patient outcomes, highlight the importance of KSAs in nursing education and for new nurses as they transition to practice. Nurses working in various clinical settings will encounter numerous opportunities for critical thinking, including:
- problem-solving, decision-making, or judgment
- patient or caregiver safety
- diagnostic reasoning (understanding and applying the nursing process)
- delivering patient-centered care
- applying moral and ethical reasoning
- applying EBP to deliver care
- using electronic medical data
- personal self-improvement, stress management, or health promotion
- improving patient outcomes and care delivery systems through quality improvement (Alfaro-Lefevre, 2019)
Given the complexity of the clinical environment, memorization-style thinking is insufficient to equip nurses with the skills to sort, organize, and interpret relevant information for effective and safe patient care. Instead, nurses must work with a broad knowledge base to individualize patient care across various clinical settings. Nursing education provides the foundation for critical thinking through experiences, reflection, communication, and observations. Then, clinical experience further develops critical thinking skills for new graduate nurses. Nurses encounter critical thinking and reflection opportunities when interacting with health and illness in the clinical setting. Nurses need to use the knowledge obtained in nursing school and clinical practice to create knowledge connections that foster critical thinking. Clinical reasoning occurs when nurses apply critical thinking by integrating theoretical knowledge with actual clinical experience. Nurses who are inquisitive and actively involved in their learning are more likely to develop clinical judgment successfully (refer to Table 1; Henshaw & Rassilyer-Bomers, 2023).
Table 1
Characteristics That Foster Critical Thinking and Clinical Reasoning
Critical Thinking | Clinical Reasoning |
|
|
(Griffits et al., 2017; Henshaw & Rassilyer-Bomers, 2023)
Clinical Decision-Making Process
Nurses use clinical judgment to make decisions based on the critical reflection of data obtained from a clinical situation. Ensuring safe, high-quality, patient-centered care requires that nurses make sound clinical judgments. New graduate nurses may take several years to develop clinical competence and sound clinical judgment. However, experienced nurses have an internalized ability to assess, apply knowledge and intuition, provide intentional thought in a situation, and collaborate with their peers and health care team to deliver safe and effective care (Zainal et al., 2025). A clinical decision-making process can help new nurses analyze data and use nursing knowledge to make clinical judgments (refer to Figure 1). The clinical decision-making process provides a framework for organized analysis of a clinical issue or problem and the selection of appropriate actions (Assessment Technologies Institute [ATI], n.d.). The steps of the clinical decision-making process include the following:
- identifying a clinical/patient issue or problem
- analyzing and interpreting relevant data
- making inferences based on the interpretation of data
- listing possible actions to be taken
- evaluating each action
- selecting the best action (ATI, n.d.)
Priority-Setting Frameworks
Nurses must apply clinical judgment when making decisions about the rank order in which nursing actions should be completed. Priority-setting frameworks are taught in nursing school to assist nurses in making decisions about priority findings, priority nursing actions, and the proper order of those actions. Nurses must continuously set and reset priorities to maintain safety and meet the needs of multiple patients. Establishing priorities requires that nurses make decisions based on data obtained during shift reports, communication with the health care team, health record review, and assessment data (ATI, n.d.; Jessee, 2019; Open Resources for Nursing, 2024). Seven priority-setting frameworks can be applied when using the clinical decision-making process to make sound clinical judgments, including:
- airway, breathing, and circulation (ABCs)
- Maslow’s hierarchy of needs
- nursing process
- safety and risk reduction
- least restrictive/least invasive
- survival potential
- acute/urgent/unstable versus chronic/nonurgent/stable (ATI, n.d.; Jessee, 2019; Open Resources for Nursing, 2024)
Airway, Breathing, Circulation
The ABC framework identifies the order of the three basic needs for sustaining life. Nurses should apply the concept of ABCs to each patient situation. Prioritization begins with determining immediate threats to life as part of the initial assessment and is based on the ABC mnemonic, focusing on the airway as the priority, then breathing, and, finally, circulation. An open airway is necessary for breathing, and breathing is necessary to oxygenate the blood. Finally, circulation is necessary for oxygenated blood to reach the body’s tissues and vital organs. The framework applies to most situations; the basic life support framework has been changed to CAB: circulation, airway, breathing (ATI, n.d.; Ignatavicius et al., 2023; Open Resources for Nursing, 2024).
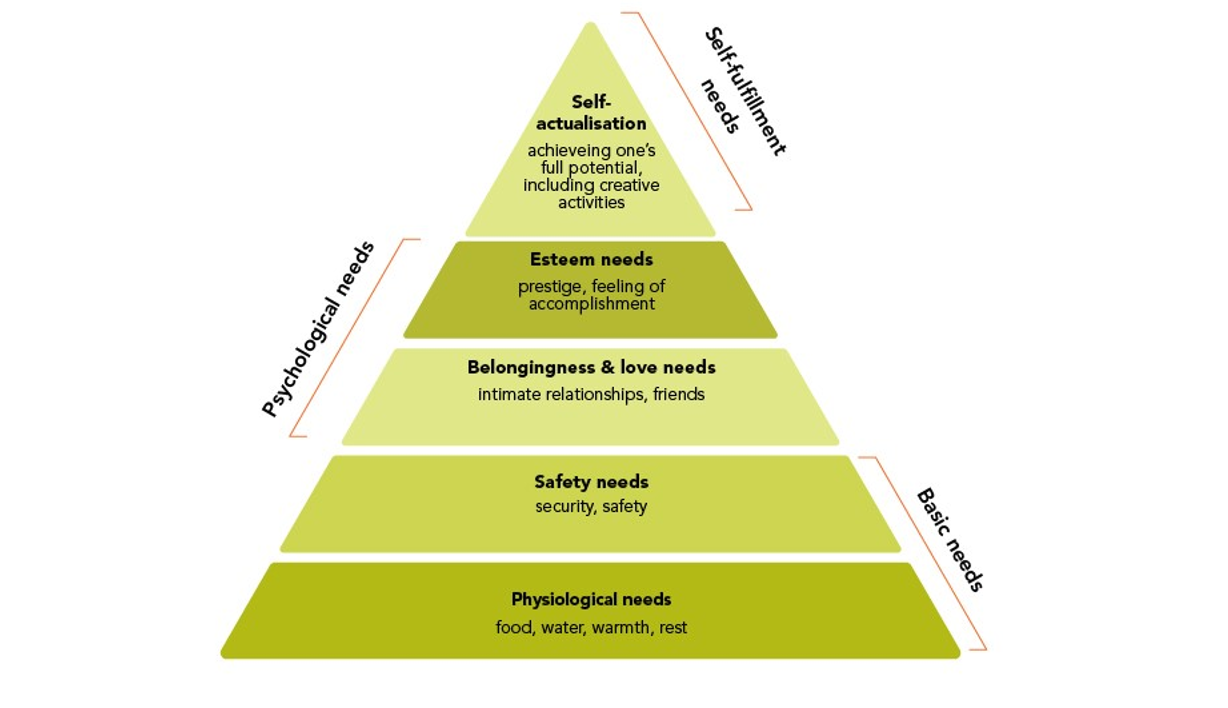
Maslow’s Hierarchy of Needs
Abraham Maslow was a psychologist who created the hierarchy of needs triangle to demonstrate human needs and their order of importance. According to this theory, all humans are born with instinctive needs, and the lower needs on the triangle must be met prior to those higher on the triangle (refer to Figure 2). If basic needs are not met to some degree, the higher-level needs will not likely be met. A person is not motivated by all five levels simultaneously; therefore, the category most relevant to the person’s current circumstances will be the primary motivator. Meeting these needs is a dynamic process that involves resolving, progressing beyond, and returning to specific levels of need. The five levels of Maslow’s hierarchy of needs include (ATI, n.d.; Henshaw & Rassilyer-Bomers, 2023; McLeod, 2026; Open Resources for Nursing, 2024):
- Physiologic needs (e.g., food, water, sleep, thermoregulation, elimination) are fundamental motivating forces. Nurses must assess each patient’s ability to meet these needs and identify nursing interventions necessary to enable patients to meet these needs.
- Safety and security (e.g., shelter and freedom from danger or harm) are also dominant motivators. Individuals need to be physically safe and free from the anxiety that results from a lack of security.
- Love and belonging (e.g., friends, intimate relationships) is the third level. To fulfill this need, a person must give and receive love.
- Esteem needs (e.g., feelings of accomplishment) are the fourth level, including self-esteem and esteem derived from others. Individuals need to know that others think well of and respect them. Self-esteem is a person’s sense of their own adequacy and worth.
- Self-actualization (i.e., achieving one’s full potential) is the fifth level and refers to the innate need to realize all of one’s abilities fully.
The bottom four levels are recognized as deficiency needs; the top level, self-actualization, is known as “being” needs; this level is not achieved by everyone. During patient care, the nurse should focus on the lower-level needs when prioritizing care. Basic physiologic and safety needs are requirements for positive patient outcomes (ATI, n.d.; McLeod, 2026; Open Resources for Nursing, 2024).
Figure 1
Nursing Process

Nursing Process
The nursing process, a systematic problem-solving approach for designing and implementing individualized care, is the foundation of the nursing profession. The nursing process can be used across all care settings with patients of all ages to identify and treat potential or actual health problems while incorporating each patient’s unique aspects. The process is dynamic and cyclical, supporting EBP to guide decision-making. The nursing process has five phases (refer to Figure 1; Henshaw & Rassilyer-Bomers, 2023; Ignatavicius et al., 2023):
- Assessment evaluates a patient’s health, including the physical, psychological, sociocultural, emotional, and spiritual factors that may impact that health state.
- Diagnosis is the clinical act of identifying problems by analyzing assessment information and deriving meaning from the findings (i.e., nursing diagnosis).
- Planning is working collaboratively with the patient to identify goals and intervention strategies to address priority problems. The written care plan provides a summary of the care the patient is to receive.
- Implementation is the action phase of the nursing process when the nurse initiates the plan of care, documenting the nursing interventions and the patient’s response to the interventions.
- Evaluation refers to the rating, grading, and judging of whether the patient’s care plan was successful.
Figure 2
Maslow’s Hierarchy of Needs
For expert nurses, the ability to prioritize based on these processes is predominantly intuitive, and tasks are completed in a prioritized manner without much conscious thought. In unfamiliar situations, patient prioritization should be approached as a structured process, highlighting risk factors contributing to a decline in the patient’s condition and potential interventions that can reduce the risk of adverse outcomes. Too often, a failure to recognize important patient data or an inability to interpret findings due to a foundational knowledge deficit can lead to adverse events. The nurse may not realize the implications until it is too late. Failure to rescue or failure to recognize and act early during a patient’s decline can result in avoidable morbidity or mortality. Seasoned nurses can pull from their depth of knowledge and experience, which allows them to act deductively and intuitively when prioritizing patient care. The novice nurse or one unfamiliar with a condition or patient situation has less experience to pull from and works from a more rigid knowledge base derived from textbook situations that may not mirror the current patient concerns. Practice and experience are the foundations of prioritizing patient care (ATI, n.d.; Henshaw & Rassilyer-Bomers, 2023; Jessee, 2018, 2019; Open Resources for Nursing, 2024).
Safety and Risk Reduction
The safety and risk reduction framework prioritizes the factor or situation that poses the most significant risk to the safety of a patient or patients. When a patient is experiencing more than one risk, the one that poses the most significant threat is deemed the highest priority. The nurse should pay particular attention to risks to the patient’s physical or psychological well-being (ATI, n.d.; Open Resources for Nursing, 2024).
Least Restrictive/Least Invasive
The least restrictive or invasive framework prioritizes nursing interventions that are least restrictive or invasive to the patient. This framework is often applied to patients exhibiting behaviors that could result in harm to the patient or caregiver or in situations when an intervention will compromise the natural barriers between the patient and the environment. When choosing the appropriate intervention, the nurse must ensure that it will not put the patient at risk of harm or injury. For example, a nurse is caring for a patient with an altered mental status who has been climbing out of bed. Utilizing this framework, the nurse should implement the least restrictive intervention, for example, moving the patient to the nurse’s station instead of applying restraints. Similarly, for a patient with incontinence, bladder training is less invasive than inserting an indwelling catheter (ATI, n.d.; Open Resources for Nursing, 2024).
Survival Potential
Survival potential is a priority-setting framework that should be applied in disaster or mass casualty incidents when the number of patients overwhelms the available resources. The principle behind this framework is to do the greatest good for the greatest number of patients. Nurses must consider the appropriate use of human and physical resources when those resources are limited. With this START framework (Simple Triage And Rapid Treatment), a patient with a limited likelihood of survival, even with intense interventions, should be assigned the lowest priority (expectant). The order of priority from highest to lowest in these situations includes Emergent (red), Urgent (yellow), Nonurgent (green), and Expectant (black; ATI, n.d.; Open Resources for Nursing, 2024; US Department of Health and Human Services, 2026).
Acute/Urgent/Unstable Versus Chronic/Nonurgent/Stable
This framework requires nurses to consider various situations and determine whether an alteration in health is acute or chronic, whether a need is urgent or nonurgent, or whether a patient is stable or unstable. Nurses must assess a patient or situation and determine if an alteration in health is a chronic condition that usually develops over time, compared to an acute change. Nurses should prioritize acute conditions over chronic conditions unless a complication is occurring. Similarly, urgent needs are given a higher priority than nonurgent ones because they threaten the patient more. This framework can be applied when the nurse is caring for multiple patients and must determine which patient to assess first. Urgent can also apply to time-sensitive nursing interventions, such as a medication due at a specific time. Unstable patients are also given priority over stable patients because their needs may pose a risk to survival. This framework can also be used for patients whose vital signs or laboratory values indicate that the patient is at risk of becoming unstable (ATI, n.d.; Open Resources for Nursing, 2024).
Principles of Delegation
Utilizing the nursing process, nurses must assess and analyze the patient or situation, identify care needs, and create a plan to set priorities for nursing actions. Finally, the nurse will perform and evaluate the response to nursing interventions during the implementation and evaluation steps of the nursing process. Assigning, delegating, and supervising are skills that the nurse may need to utilize to manage the needs of the assigned patients. In order to utilize these skills, the nurse must understand the difference between these terms (ATI, 2023; Henshaw & Rassilyer-Bomers, 2023).
- Assigning refers to transferring authority, accountability, and responsibility of patient care to another health care team member.
- Delegating refers to transferring the authority and responsibility of a task to another health care team member while retaining accountability.
- Supervising refers to directing, monitoring, and evaluating the performance of tasks completed by another health care team member. Registered nurses (RNs) are responsible for supervising tasks that are delegated to a licensed professional nurse (LPN) or unlicensed assistive personnel (UAP).
Nurses must assign, delegate, and supervise appropriately, following the ANA professional standards, health care facility policies, and state nurse practice acts. Assigning occurs in a downward or lateral manner to another health care team member (ATI, 2023; Henshaw & Rassilyer-Bomers, 2023). When assigning, the nurse should consider various factors, including
- condition of the patient and level of care
- need for specific precautions (e.g., seizure, fall, isolation)
- specific care needs (e.g., cardiac monitoring, wound care)
- knowledge and skill of the team member
- staffing mix (i.e., RN, LPN, UAP)
- nurse-to-patient ratio
- experience of staff with similar patients
- amount of supervision required (ATI, 2023; Henshaw & Rassilyer-Bomers, 2023)
Delegation
An RN can delegate to other RNs, LPNs, and UPAs, while an LPN can delegate to other LPNs and UAPs. Nurses should delegate only tasks that are appropriate for the knowledge and skill of the health care team member they are delegating to (refer to Table 2). In addition, nurses must provide clear directions when a task is initially delegated and for periodic reassessment and evaluation. RNs cannot delegate patient education, key components of the nursing process (assessment, planning, and evaluation), or tasks that require clinical judgment (ATI, 2023; Henshaw & Rassilyer-Bomers, 2023). The delegating nurse must consider the following:
- task factors
- potential for harm (i.e., bleeding, aspiration, fall)
- predictability of outcome (i.e., whether it is a routine treatment with a predictable outcome)
- need for problem-solving and innovation (i.e., clinical judgment or assessment)
- complexity of care (i.e., whether the delegatee is qualified to perform the skill)
- level of interaction with the patient (i.e., whether education is required)
- delegatee factors
- knowledge, training, and experience
- demonstrated competence
- institutional policies and licensing legislation
- ability to communicate with others
- five rights of delegation
- right task (i.e., the task should be appropriate and require minimal supervision and risk of harm)
- right circumstance (i.e., assess the complexity of care and match this to the skill level of the delegatee)
- right person (i.e., assess and verify the delegatee’s scope of practice, training, and competence)
- right direction/communication
- data to be collected
- specific task to be performed
- method and timeline for reporting concerns or findings
- expected results
- right supervision/evaluation
- provide supervision directly or indirectly (i.e., assign to another licensed nurse)
- monitor performance
- provide feedback
- evaluate the patient and determine if outcomes were met
- intervene if necessary (i.e., unsafe practices; ATI, 2023; Henshaw & Rassilyer-Bomers, 2023)
Table 2
Tasks Appropriate for Delegation From an RN to an LPN or UAP
LPN | UAP |
Reinforcing patient teaching from a care plan | Activities of daily living (ADLs; bathing, grooming, dressing, toileting) |
Tracheostomy care or suctioning | Ambulating |
Monitoring findings (input for the RN’s assessment) | Feeding (excluding aspiration precautions) |
Inserting a urinary catheter | Positioning |
Checking nasogastric tube patency | Intake and output |
Administering enteral feedings | Vital signs (for stable patients) |
Administering medication (excluding first-dose intravenous [IV] medications in some states) | Specimen collection |
(ATI, 2023; Henshaw & Rassilyer-Bomers, 2023; NCSBN, n.d.)
Case Studies for Prioritization Practice
Case Study 1
A medical-surgical nurse who has been practicing on their unit for 2 years has been asked to work in the emergency department with the following patients. In what order should they treat the following patients, and why?
- CM is a school-aged child with a 2 cm laceration to the left arm. The laceration is bleeding through a 4 × 4 gauze every 5–10 minutes
- SC is a young adult reporting a headache (pain rates as 9 out of 10), vomiting, and inability to open their eyes due to light sensitivity
- GF is an adult with a history of chronic obstructive pulmonary disease (COPD) and has reported increased breathing difficulty for the past 2 hours. They also report a recent cold with significant worsening in the past 24 hours
- LH is an adult with intermittent chest pain for 2 days who currently rates their pain as 5 out of 10 (LaCharity et al., 2025)
Answer Key: Case Study 1
The nurse must utilize a priority-setting framework to determine which patient should be evaluated first. Utilizing the ABCs framework, the nurse should treat the patients in this order:
(c) An adult with COPD and increased difficulty breathing for the past 2 hours. The patient reports a recent cold has worsened significantly in the past 24 hours. This patient is a priority due to breathing in the ABC framework.
(d) An adult with intermittent chest pain for 2 days who currently rates the pain as 5 out of 10. This patient could be experiencing a myocardial infarction (MI), and care should be initiated promptly before their condition declines.
(a) A child with a 2 cm laceration to their left arm. The laceration is bleeding through a 4 × 4 gauze every 5–10 minutes. This patient would take priority over pain since they were bleeding, even with a small amount of bleeding.
(b) A young adult reporting a headache (9 out of 10), vomiting, and inability to open their eyes due to light sensitivity. While the patient has pain, their condition is not considered life-threatening (LaCharity et al., 2025).
Case Study 2
A travel nurse is given a 4-hour orientation to the unit they are working on today. They receive a report on the six patients they will care for during the shift. Which of the following nursing actions should be the priority?
- Ensure they have access to the unit’s computer and medication dispensing systems
- Develop a schedule for lunch and breaks in collaboration with the other staff
- Request a bedside report rather than the current reporting system at this facility, since this is what they are used to
- Ensure that they know where the policy and procedure manual is located
- Identify a contact person on the unit that can provide additional information if needed (LaCharity et al., 2025)
Answer Key: Case Study 2
The nurse’s first priority should be ensuring access to the unit’s computer and medication dispensing systems to deliver proper patient care (a). The second priority would be determining a contact person to help with additional needed information (e), followed by the policy and procedure manual (d). Each of these can help them provide care for their patient assignment. Developing a schedule is a great way to organize for the day (b). It would be appropriate to ask for a bedside report, and if the reporting nurses are not opposed, then this style of hand-off can be utilized (c; LaCharity et al., 2025).
Case Study 3
A nurse with 6 months of experience has recently completed orientation on their unit. They are caring for five patients today. The following report was given about their patients. Which patient should they assess first?
- An adult patient who is 4 hours postcholecystectomy with uncontrolled pain
- A young adult with newly diagnosed type 1 diabetic and a blood sugar of 320
- An adolescent patient who attempted suicide with acetaminophen (Tylenol) last night and is being transferred to a psych unit this afternoon
- An older adult patient with Alzheimer’s disease, increased confusion, and right-sided weakness that started approximately 1 hour ago
- An adult patient who had an MI last night and is going to surgery in 1 hour (LaCharity et al., 2025)
Answer Key: Case Study 3
The nurse should assess the older adult patient with Alzheimer’s who has increased confusion and right-sided weakness that started approximately 1 hour ago (d). This patient may be experiencing a stroke and requires immediate care. In this scenario, the nurse is applying the safety and risk reduction framework. According to the report, the patient who had an MI last night (e) is already scheduled for surgery and is likely stable. While all patients need to be seen as soon as possible, this is the priority due to the limited window for interventions with potential stroke (LaCharity et al., 2025).
Case Study 4
A travel nurse is on a 4-week level 1 trauma center assignment as a critical care unit nurse. They are in their second week and feel comfortable with the unit and the staff. They have two patients. Patient A is an adult who is 12 hours status-post coronary artery bypass graft, and patient B is an adult who was in a motor vehicle accident 36 hours ago and has multiple fractures and a flail chest. The nurse should complete the following tasks related to their care in which order?
- morning assessments
- administer PRN pain medication to patient B
- take the report from the night nurse
- adjust patient A’s medications based on the provider’s orders and the most recent set of lab results
- call the provider about patient B’s morning lab results
- review the medication administration record (MAR) and create a medication administration schedule for both patients
- empty the Jackson-Pratt (JP) drains in patient A’s chest
- personal care (bathing and oral care) for both patients (LaCharity et al., 2025)
Answer Key: Case Study 4
(c) Take report from the night nurse
(a) Morning assessments
(b) Administer PRN pain medication to patient B
(e) Call the provider about patient B’s morning lab results
(d) Adjust patient A’s medications based on the provider’s orders and the most recent lab results
(f) Review the MAR and create a medication administration schedule for both patients
(g) Empty the JP drains in patient A’s chest
(h) Personal care (bathing and oral care) for both patients
First, obtaining the report from the previous shift’s nurse is important to apply a priority-setting framework. A patient assessment can follow this to ensure the patient’s status matches the report (nursing process). Since patient B has pain, it is important to address that before the other activities listed. Likely, the PRN pain medication would be administered during the morning assessment after ensuring there are no other reasons for the pain and that it is appropriate to give at this time. After this, the provider should be notified of patient B’s labs to allow any medications or treatments to be adjusted. Most nurses create a medication schedule at the start of their shift to avoid missing administration times. Unless patient A’s JP drains are full or leaking, they can wait to be emptied until the other activities have been done. Just before personal care is a good time to empty drains and assess wounds, while dressing changes are usually done immediately after personal care (LaCharity et al., 2025).
Case Study 5
The nurse is working in a pediatric unit today and has six patients. They are working with a health care team that includes a UAP, an LPN, and a respiratory therapist (RT) on call. The following patients and diagnoses are assigned to them:
- a 6-year-old returning from tonsillectomy needing PRN intramuscular (IM) or oral (PO) pain medication
- a 4-year-old with an asthma exacerbation needing their respiratory treatment
- a 10-month-old who is status-post pyloromyotomy for pyloric stenosis and needs a bath
- a 12-year-old who had a 4-wheeler accident 2 days ago, resulting in a fractured femur and multiple wounds, who needs a dressing change for an arm wound
- a 14-year-old who is 12 hours post-appendectomy for an appendix rupture, reporting nausea
- a 4-month-old with respiratory syncytial virus needing their nose cleared of drainage (LaCharity et al., 2025)
Consider the following:
- Which patient(s) would be appropriate to delegate to the UAP?
- Which patient(s) would be appropriate to delegate to the LPN?
- Which patient(s) would be appropriate to call RT?
- Which patient should the nurse assess first, and why?
Answer Key: Case Study 5
(1) The UAP can manage the bath for the 10-month-old (c). Using UAPs for personal care activities is an appropriate delegation of duties.
(2) The LPN can manage the PRN pain medication that is either IM or PO for the 6-year-old post-tonsillectomy patient (a), the dressing change for the arm wound (d), and the 4-month-old nasal suctioning (f; typically, with a bulb syringe).
(3) The RT could be contacted to determine if they can administer the respiratory treatment (b).
(4) The nurse should assess the 14-year-old reporting nausea after surgery for a ruptured appendix (e) as the patient could be having a complication related to their surgery and should be fully assessed by the nurse quickly (LaCharity et al., 2025).
Case Study 6
The nurse has been assigned to the neurology floor for the first time. They typically work on a pediatric floor. They are very nervous about this assignment as they are unfamiliar with this type of patient. The charge nurse assigns them five patients and gives them a shift report. Which of the following should be of greatest concern to this nurse?
- An adult patient who had a brain aneurysm repaired 2 days ago. The patient just arrived at the neuro unit from the intensive care unit and is reportedly stable with occasional reports of pain. The patient has an IV in the left antecubital with half-normal saline (0.45% NaCl) infusing and an IV in the right forearm that is heparin locked with flushes every shift. The UAP tells the nurse that the patient is comfortable but that their IV pump is “going off” and the fluid bag looks low.
- An adult patient who had a stroke and has a platelet level of 250,000 µ/L on their most recent set of labs. The patient is resting comfortably in bed and watching television. The patient’s morning medications are due, and their urinary catheter needs to be removed.
- An adult patient who was admitted yesterday with an exacerbation of a seizure disorder. The patient had a valproic acid (Depakene) level of 75 µ/L this morning. The patient has not had their morning medications, including their valproic acid (Depakene), and is currently eating breakfast.
- An adult patient with a brain tumor and a history of seizures on phenytoin (Dilantin) with a current level of 28 mg/dL. The patient is asleep and has asked to be left alone.
- An adult patient with multiple sclerosis (MS) who is receiving prednisone (Deltasone) IV. The patient’s steroid dose was due 1 hour ago, but their IV needs to be restarted as it was pulled out overnight. The patient is currently in the shower with the assistance of a UAP (LaCharity et al., 2025).
In what order should the nurse assess these patients?
Answer Key: Case Study 6
The nurse should be most concerned about the adult patient with a phenytoin (Dilantin) level of 28 mg/dL (d), significantly higher than the therapeutic level of 10-20 mg/dL. Phenytoin (Dilantin) toxicity can have serious implications; the patient should be evaluated, and the provider should be notified promptly. This should be the priority among this group of patients, as the other patients are currently stable. The nurse can use the safety and risk reduction framework or the acute/urgent/unstable versus chronic/nonurgent/stable framework.
They should assess the other patients in the following order:
(a) The recent transfer who needs their IV checked to either replace the fluid bag or troubleshoot why the alarm is sounding
(e) The patient with MS to restart their IV and initiate their medication
(b) The patient who needs medications and to discontinue their urinary catheter
(c) The patient with a valproic acid (Depakene) level of 75 µ/L, which is normal for a morning assessment (LaCharity et al., 2025)
Case Study 7
An agency nurse is assigned to an acute care unit in a long-term care (LTC) facility. The nurse receives a report on their patients for the day. Whom should they assess first after receiving the report?
- A resident with congestive heart failure (CHF) and 3+ pitting edema in their bilateral lower extremities
- A resident with Parkinson’s disease (PD) who started hallucinating during the night and is now sleeping
- A resident with Alzheimer’s disease who was wandering in the hallway at 2 a.m.
- A resident with terminal cancer, whom the UAP reported has lost 8 lb since their last weight check 4 weeks ago
Answer Key: Case Study 7
In the LTC setting, many patients have chronic, stable conditions. Therefore, the nurse must prioritize which patient to assess first by considering if there is a risk to safety or an acute or unstable patient. Based on this, the nurse should treat the patients in the following order:
(b) The patient with PD who experienced hallucinations during the night should be assessed first. This patient may be experiencing an adverse reaction to their PD medications. The other patients’ symptoms are consistent with their conditions.
(a) The second patient would be the CHF patient, as 3+ pitting edema may require a medication adjustment, but this type of edema is expected with CHF.
(d) Significant weight loss is expected in patients with terminal cancer. However, this patient should be next to assess for acute needs.
(c) It is not abnormal for a patient with Alzheimer’s to wander at night, which is a stable situation (LaCharity et al., 2025).
After the nurse completes their morning assessments, they review the MAR and note that they have several medications to give. Which of the following medications should be given first, and why?
- Acyclovir (Zovirax) for a resident diagnosed with Bell’s palsy
- Cephalexin (Keflex) for a resident diagnosed with a urinary tract infection
- Acetylsalicylic acid (Aspirin) for a resident diagnosed with cerebrovascular accident
- Neostigmine (Prostigmin) for a resident diagnosed with myasthenia gravis (MG) (LaCharity et al., 2025)
The medication priority would be:
(d) Neostigmine (Prostigmin) promotes muscle function in patients diagnosed with MG. This medication should always be administered on time to prevent loss of muscle tone, especially in the upper respiratory tract muscles. Therefore, this would be the priority medication to administer at this time. The remaining medications can be administered 30 minutes before or after their scheduled time without implications, so none of these are considered priority medications (LaCharity et al., 2025).
Case Study 8
The nurse just took a job as a home health nurse, and today is their first day off of orientation. They have four patients. Which of them should they visit first, and why?
- A patient with a new diagnosis of MS, who stated to their family member that they are depressed
- A patient with PD who is walking with a short, shuffling gait, as reported by their caregiver
- A patient with a recent C5 spinal cord injury whose family member reports redness and drainage at the Halo vest sites
- A patient with a low back injury (L4), who called the office, reporting a severe headache (LaCharity et al., 2025)
Answer Key: Case Study 8
(c) The patient with a recent C5 spinal cord injury reporting redness and drainage at the insertion sites of the Halo vest is the priority. The Halo vest is inserted into a bone, and an infection around the insertion site can lead to osteomyelitis. This could become life-threatening and should be investigated immediately.
(d) The next priority would be the patient with a low back (L4) injury reporting severe headaches. This would be a more urgent concern if the spinal injury were higher, as it could indicate autonomic dysreflexia. However, this level is less urgent and more likely to represent a rebound headache due to pain medication or a slow spinal fluid leak.
(a) The patient with MS who states they are depressed should be the next patient. The nurse would want to ensure that there is no risk of self-harm or self-injurious behavior.
(b) Finally, PD very often causes a shuffling gait; this will require education for the patient and family regarding the disease process (LaCharity et al., 2025).
Case Study 9
The nurse is performing triage in a level I trauma center. The charge nurse reports that there was a 20-car pileup on the highway with reports of numerous patients who were seriously injured. The health care facility has initiated a disaster response due to this mass casualty incident. The triage nurse must utilize the potential survival framework to color-code each patient brought into the facility. Which color designation should each of the following patients receive, and in what order should the health care team treat them?
- A 10-year-old who walks in with emergency personnel reporting left arm pain
- A 45-year-old who has a depressed skull fracture and a Glasgow coma scale (GCS) of 3 and a respiration rate of 6
- A 67-year-old with an open left-sided chest injury and absent breath sounds on that side. The patient is alert, with a respiration rate of 34
- A 23-year-old with a laceration to the left leg that is bleeding through a dressing every 10 minutes (LaCharity et al., 2025)
Answer Key: Case Study 9
The goal of applying the survival-potential framework is to help the most patients when resources are limited. With this framework, a patient with a minimal chance of survival would be given the color black (signifying they are expectant) and seen last. In this scenario, the nurse should categorize and assess the patients in the following order:
(c) A 67-year-old with an open left-sided chest injury and absent breath sounds on that side. The patient is alert, with respirations of 34 (red tag/emergent).
(d) A 23-year-old with a laceration to the left leg that is bleeding through a dressing every 10 minutes (yellow tag/urgent).
(a) A 10-year-old who walks in with emergency personnel reporting left arm pain (green tag/nonurgent).
(b) A 45-year-old who has a depressed skull fracture and a GCS of 3 and respirations of 6 (black tag/expectant; LaCharity et al., 2025).
Case Study 10
The nurse has an LPN and a UAP on their health care team to assist with patient care. Which of the following tasks would be appropriate to delegate to the LPN? Which would be appropriate to delegate to the UAP?
- Assist a patient with MS in ambulating to the bathroom
- Assess a newly admitted patient with pneumonia
- Take the initial vital signs while administering a unit of blood to a patient
- Administer a vitamin B12 injection to a patient with pernicious anemia (Lacharity et al., 2019)
While many of these tasks seem simple, choosing the “next right move” or appropriately delegating can be difficult. Incorrect decisions by the nurse can lead to poor patient outcomes or even death. Upon arrival at the unit or point of care, nurses should identify and establish their care priorities, considering a rationale for each action taken in practice. They should identify and trend clinical data relevant to the patient’s condition, as these are often precursors to impending changes in condition. The ability to prioritize is built on the knowledge of patient conditions and experience. The nurse must learn to differentiate between problems that must be attended to immediately versus those that can wait. When in doubt, nurses should delegate to personnel (i.e., LPN, UAP) and resources available in the workplace, such as mentors, peers, or online resources (Jessee, 2019; LaCharity et al., 2025).
Answer Key: Case Study 10
(a) The UAP can assist the patient in ambulating to the bathroom.
(d) The LPN can administer the B12 injection to the patient with pernicious anemia.
(b, c) The nurse will need to complete the admission assessment on the pneumonia patient and take the initial vital signs during blood administration. The LPN’s role in blood administration varies among states and institutions, but typically, the RN must, at a minimum, do the initial set of vital signs and hang the blood (LaCharity et al., 2025).
References
Alfaro-Lefevre, R. (2019). Critical thinking, clinical reasoning, and clinical judgment: A practical approach (7th ed.). Elsevier.
Alharbi, H. F., Alzahrani, J., Hamed, A., Althagafi, A., & Alkarani, A. S. (2023). The experiences of newly graduated nurses during their first year of practice. Healthcare, 11(14), 2048. https://doi.org/10.3390/healthcare11142048
American Nurses Association. (2021). Nursing: Scope and standards of practice (4th ed.). https://www.nursingworld.org/practice-policy/scope-of-practice
American Nurses Association. (2024). Critical thinking in nursing: Tips to develop the skill. https://www.nursingworld.org/content-hub/resources/nursing-leadership/critical-thinking-nursing
Assessment Technologies Institute. (n.d.). Critical thinking guide. Retrieved March 5, 2026, from https://nextgen.atitesting.com/ProductOffering/Critical-Thinking-Guide/Critical-Thinking-Guide.html#
Assessment Technologies Institute. (2023). Content mastery series: Review module: Nursing leadership and management (9th ed.).
Benner, P., Tanner, C. A., & Chesla, C. A. (2009). Expertise in nursing practice: Caring, clinical judgment, and ethics (2nd ed.). Springer Publishing.
Centers for Disease Control and Prevention. (2024). Preventing chronic diseases: What you can do now. https://www.cdc.gov/chronic-disease/prevention/index.html
Centers for Disease Control and Prevention. (2025). About chronic diseases. https://www.cdc.gov/chronic-disease/about
Connor, J., Flenady, T., Massey, D., & Dwyer, T. (2022). Clinical judgement in nursing: An evolutionary concept analysis. The Journal of Clinical Nursing, 32(13-14), 3328–3340. https://doi.org/10.1111/jocn.16469
Fernaays, J. (2024). Reverse prioritization: A new approach to prioritizing in the classroom. Teaching and Learning in Nursing, 19(3), 285–287. https://doi.org/10.1016/j.teln.2024.04.013
Griffits, S., Hines, S., Moloney, C., & Nicholas, R. (2017). Characteristics and processes of clinical reasoning in nurses and factors related to its use: A scoping review protocol. JBI Database of Systematic Reviews and Implementation Reports, 15(12), 2832-2836. https://doi.org/10.11124/JBISRIR-2016-003273
Henshaw, C. M., & Rassilyer-Bomers, R. (2023). Craven’s fundamentals of nursing: Concepts and competencies for practice (10th ed.). Wolters Kluwer.
Ignatavicius, D. D., Rebar, C. R., & Heimgartner, N. M. (2023). Medical-surgical nursing: Concepts for clinical judgment and collaborative care (11th ed.). Elsevier.
Jessee, M. A. (2018). Pursuing improvement in clinical reasoning: The integrated clinical education theory. Journal of Nursing Education, 57(1), 7–13. https://doi.org/10.3928/01484834-20180102-03
Jessee, M. A. (2019). Teaching prioritization. “Who, what, & why?” Journal of Nursing Education, 58(5), 302–305. https://doi.org/10.3928/01484834-20190422-10
Kavanagh, J. M., & Szweda, C. (2017). A crisis in competency: The strategic and ethical imperative to assessing new graduate nurses’ clinical reasoning. Nursing Education Perspectives, 38, 57–62. https://doi.org/10.1097/01.NEP.0000000000000112
LaCharity, L. A., Kumagai, C. K., & Hosler, S. M. (2025). Prioritization, delegation, and assignment: Practice exercises for the NCLEX-RN examination (6th edition). Elsevier.
Manetti, W. (2019). Sound clinical judgment in nursing: A concept analysis. Nursing Forum, 54, 102–110. https://doi.org/10.1111/nuf.12303
McGarity, T., Monahan, L., Acker, K., & Pollock, W. (2023). Nurse graduates’ preparedness for practice: Substantiating the call for competency-evaluated nursing education. Behavioral Sciences, 13(7), 533. https://doi.org/10.3390/bs13070553
McLeod, S. (2026). Maslow’s hierarchy of needs. https://www.simplypsychology.org/maslow.html
Mohamed, Z., & Al-Hmaimat, N. (2024). The effectiveness of nurse residency programs on new graduate nurses’ retention: Systematic review. Heliyon, 10(5), e26272. https://doi.org/10.1016/j.heliyon.2024.e26272
National Council of State Boards of Nursing. (n.d.). Delegation. Retrieved March 8, 2026, from https://ncsbn.org/nursing-regulation/practice/delegation.page
National Council of State Boards of Nursing. (2019). The next generation NCLEX project. https://www.yearinreview2019.ncsbn.org/stories/07-2019
National Council of State Boards of Nursing. (2023). NCSBN launches next generation NCLEX exam. https://www.ncsbn.org/news/ncsbn-launches-next-generation-nclex-exam
Nursing Education Staff. (2024). Nurse insights: How can nurses develop clinical judgment? https://nursingeducation.org/insights/clinical-judgment
Open Resources for Nursing (Ed.). (2024). Nursing management and professional concepts (2nd ed.). Chippewa Valley Technical College. https://www.ncbi.nlm.nih.gov/books/NBK610445
Quality and Safety Education for Nurses. (n.d.). QSEN institute competencies. Retrieved March 3, 2026, from https://qsen.org/competencies/graduate-ksas
Rebelo, A. (2020). How prepared are new nurse graduates for practice today? Clinical judgment skills identified as a primary gap in practice readiness according to Wolters Kluwer report. https://www.wolterskluwer.com/en/news/how-prepared-are-new-nurse-graduates-for-practice-today
Rose, K. (2022). Creative tips for teaching clinical judgment. https://www.wolterskluwer.com/en/expert-insights/creative-tips-teaching-clinical-judgment
US Department of Health and Human Services. (2026). START adult triage algorithm. https://remm.hhs.gov/startadult.htm
Yingnan, Z., Ziqi, Z., Ting, W., Liqin, C., Xiaoqing, S., & Lan, X. (2024). Transitional shock in newly graduated registered nurses from the perspective of self-depletion and impact on cognitive decision-making. Journal of Nursing Management, 2024, 6722892. https://doi.org/10.1155/2024/6722892
Zainal, N. H., Islam, M. A., Rasudin, N. S., Mamat, Z., Hanis, T. M., Hasani, W. S. R., & Musa, K. I. (2025). Critical thinking and clinical decision making among registered nurses in clinical practice: A systematic review and meta-analysis. Nursing Reports, 15(5), 175. https://doi.org/10.3390/nursrep15050175
Powered by Froala Editor